
Whether you struggle with nausea from morning sickness, illness or you just drank too much last night, here are my top tips for cures. Take it from a girl who spends hours every day feeling sick: this stuff works!
Whether you struggle with nausea from morning sickness, illness or you just drank too much last night, here are my top tips for cures. Take it from a girl who spends hours every day feeling sick: this stuff works!
Many women take their reproductive health for granted but it can prove vital to understand your own body and identify what normal is for you. So, join us as we discuss all things related to PCOS and tackle the truth behind the taboo, with help from some genuine PCOS experiences.

With September marking Polycystic Ovary Syndrome awareness month, we believe that it is time to put a spotlight on the condition. According to NHS England, PCOS affects 1 in 5 women here in the UK but do we know enough about it?
Polycystic ovary syndrome (PCOS) is a condition which affects a woman’s hormone levels, specifically involving the production of androgen — male hormones. This imbalance can lead to irregular periods, which means that your ovaries do not release eggs regularly.
One common misconception is that having polycystic ovaries means that you have cysts — this isn’t the case. They are not true cysts in the sense that they aren’t filled with liquid and they don’t grow large and burst. In actuality they are follicles that contain immature eggs and because they have not matured enough, they don’t trigger ovulation.
The signs of PCOS will usually become apparent during a woman’s late teens or early 20’s — but it can affect women of all ages. The severity and range of symptoms experienced is likely to differ between people but some of the possible signs to look out for include:
Your GP should be your first port of call if you are worried about experiencing any of the above. The problem that many women face with PCOS is that it is often misdiagnosed with a whole array or other conditions that can mimic the symptoms. This can make the diagnosis a long, difficult process.
Niamh, 22, describes that she had ‘’experienced severe cramps that were getting in the way of my normal routines, as well as period irregularities, so I was really concerned at the time. Before the PCOS diagnosis my doctor suggested trying over the counter painkillers but after few trips back to the surgery I was finally told that I had the condition’’.
Get familiar with what is normal for you and your body and if you are concerned about anything then be sure to make an appointment with your GP. Irregular or heavier periods are some of the most common symptoms of PCOS and managing them from month to month can be difficult. Your period shouldn’t get in the way of your normal routine, so make sure you look for the right product for you, with the correct absorbency for your flow. You could try using tampons for heavy periods, as they are available in the widest range of absorbencies. By finding the absorbency that suits your individual flow, you won’t have to worry about leaks.
Whilst there is no cure for PCOS, after a woman is diagnosed with the condition the symptoms can be managed and relieved through multiple approaches. Various medications might be prescribed by a doctor following diagnosis: Clomifene is usually the first option prescribed to help ovulation resume, or Metformin (used commonly to treat type 2 diabetes) can be given to women — although for PCOS it is used ‘off-label’ as it isn’t actually licensed for treating the condition in the UK. There’s also medication options for targeting other PCOS symptoms such as acne and unwanted hair loss/ growth.
Becca, 24, spoke about the treatment options following her PCOS diagnosis, saying that ‘’People are very unaware of how different the symptoms can be, and treatment needs to be quite personalised’’. As well as the options we’ve discussed, there are treatments based on naturopathy that women could opt for. For PCOS it is important that as women, we deconstruct the ‘one size fits all’ approach to managing the symptoms, both visible and not. Becca added that ‘’it is possible for treatments to mask your symptoms rather than alleviate the root of the problem — and some women don’t even get a PCOS diagnosis before they’re offered medication for the signs’’.
For many women, fertility after a PCOS diagnosis is a big concern but the outcome isn’t always negative. With treatment in place, getting pregnant naturally is possible and there are multiple medications that are commonly prescribed to treat symptoms and stimulate fertility.
A fertility specialist will be able to provide more guidance for women who have PCOS and struggle to conceive naturally. However, you can take positive steps to manage symptoms and boost fertility, including modifying your diet and lifestyle. Unfortunately, some women do require further help to get pregnant in PCOS cases and in vitro fertilization might be recommended.
However, it’s important to remember that PCOS doesn’t affect fertility in the same way for all women with the condition and natural pregnancies are possible!
September is PCOS Awareness Month, but do we know enough about how it affects our bodies and do we feel that it is approached in the right way? Jade, 23, described her frustration during her PCOS diagnosis, saying ‘’From my experience, PCOS isn’t treated with enough sensitivity and as few of the symptoms are visible, people can often pass it off as period pain which makes you feel invalid’’. She adds that she ‘’went through so many tests, from bloods to thyroid examinations, with no clear diagnosis, it felt like I was just being passed back and forth between doctors’’.
As the signs of PCOS affect everyone differently, there is a vast spectrum for experiencing the condition and you might only notice one or two mild symptoms. All of the women that we spoke to expressed an unawareness of the condition prior to their diagnosis and this poses the issue of education — should schools be sharing more with their female students on this, in order to develop better understandings of our intimate health? Tackling a taboo of this nature is essential in helping women normalise their experiences and seek the right guidance and healthcare.
So, let’s all become more PCOS aware this September and as always — know what is normal for your body and don’t be afraid to voice any concerns!
https://www.nhs.uk/conditions/polycystic-ovary-syndrome-pcos/symptoms/
https://www.healthline.com/health/polycystic-ovary-disease
https://www.self.com/story/pcos-and-endometriosis-causes-symptoms-and-treatment
https://www.pcosoracle.com/celebrities-with-pcos/
https://helloclue.com/articles/cycle-a-z/deep-diagnosis-a-naturopathic-approach-to-pcos
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1334192/
https://moodymonth.com/articles/what-is-polycystic-ovary-syndrome-pcos-and-how-can-you-treat-it
https://www.glamour.com/story/living-with-pcos-taught-me-to-redefine-my-standards-of-beauty

Morton’s neuroma
Morton’s neuroma is a painful foot condition that affects one of the nerves between the toes.
It’s also known as Morton’s metatarsalgia or interdigital neuroma.
In Morton’s neuroma, a nerve in the foot becomes irritated and thickened, which can cause severe pain.
The condition can occur in one foot or both feet. It usually affects the nerve between the third and fourth toes, but sometimes the second and third toes are affected.
Morton’s neuroma can occur at any age, but most often affects middle-aged women. This may be because women tend to wear tight or high-heeled shoes that can put pressure on the feet.
It’s also increasingly seen in runners, possibly because of the increased pressure on the toes that occurs when running.
You may initially experience a tingling sensation in the space between your toes, which gets worse over time. This eventually develops into a sharp shooting or burning pain in the ball of your foot or at the base of your toes. There may also be some numbness in your toes.
The pain is often worse when walking or wearing shoes that squash the feet. Some people describe walking with Morton’s neuroma as feeling like there’s a small stone stuck under your foot. Removing your shoes and rubbing your foot may reduce the pain.
It’s a good idea to make an appointment to see a podiatrist (specialist in foot problems) if you have persistent symptoms of Morton’s neuroma, as the condition is unlikely to improve on its own. You could also visit your GP, who may refer you to a podiatrist.
Your GP or podiatrist may examine your foot and ask you some questions to find out:
about the pain and what it feels like
when your symptoms started
what type of shoes you usually wear
about your work, lifestyle and sporting activities
They can also suggest simple measures you can try at home to reduce your symptoms, or recommend other treatments.
Find a podiatrist near you.
Morton’s neuroma occurs when one of the nerves between the toe bones becomes irritated, which causes it to become thicker. The exact cause of the irritation is unknown, but it may be caused by the nerve being squashed (compressed), stretched or damaged.
The condition has been linked to:
wearing tight, pointy or high-heeled shoes
being active and playing sport – particularly running or sports that involve running and placing pressure on the feet, such as racquet sports
other foot problems, such as flat feet, high arches, bunions and hammer toes
It’s not clear if these directly cause the condition or just make the symptoms worse.
Treatment for Morton’s neuroma will depend on how long you’ve had the condition and its severity. Simple non-surgical treatments are effective for some people. Others may need surgery.
At first, your podiatrist or GP may recommend:
changing your footwear – shoes with a wider toe area may help ease the pressure on the nerve in your foot
orthotic devices – a soft pad for the ball of your foot may help relieve the pressure on the nerve
painkillers – taking over-the-counter anti-inflammatory painkillers, such as ibuprofen, may help ease the pain and inflammation
losing weight – if you’re overweight, losing weight may reduce the strain on your feet
injections – injections of a steroid medication or alcohol solution alongside a local anaesthetic may offer some pain relief
Resting your foot and massaging your toes may also help relieve the pain. Some people also find it useful to hold an ice pack against their foot.
A relatively new procedure called cryosurgery (or cryotherapy), where a small probe is inserted into the foot and used to destroy the thickened nerve tissue by freezing it, is also sometimes used to treat Morton’s neuroma. However, this is still fairly experimental and isn’t widely available in the UK. You’ll usually have to pay for it privately.
Surgery for Morton’s neuroma is usually only recommended if you have very severe pain or if the treatments above haven’t worked. In this case, your GP can refer you to a podiatric or orthopaedic surgeon to discuss whether surgery is suitable for you.
During the operation, a small incision is made on the top or bottom of your foot so the surgeon can access the affected nerve. They will then either:
increase the space around the nerve by removing some of the surrounding tissue, or
remove part of the nerve – if this is done, the area between your toes will be permanently numb
The procedure is usually carried out using a general anaesthetic or local anaesthetic. You normally won’t need to stay in hospital overnight.
After the procedure, you’ll need to wear a special protective shoe until the affected area has healed enough to wear normal footwear. You can usually walk soon after the operation, although it will take weeks or months to make a full recovery.
Most people who have surgery to treat Morton’s neuroma have positive results and their pain is relieved afterwards.
As with all types of surgery, however, complications can occur, such as swelling, infection and pain. You should discuss the risks with your surgeon before having the procedure.
Klinefelter syndrome
Klinefelter syndrome (sometimes called Klinefelter’s, KS or XXY) is where boys and men are born with an extra X chromosome.
Chromosomes are packages of genes found in every cell in the body. Two types of chromosome, called the sex chromosomes, determine the genetic sex of a baby. These are named either X or Y.
Usually, a female baby has two X chromosomes (XX) and a male has one X and one Y (XY). But in Klinefelter syndrome, a boy is born with an extra copy of the X chromosome (XXY).
The X chromosome is not a “female” chromosome and is present in everyone. The presence of a Y chromosome denotes male sex.
Boys and men with Klinefelter syndrome are still genetically male, and often will not realise they have this extra chromosome, but occasionally it can cause problems that may require treatment.
Klinefelter syndrome is quite common, affecting around 1 in every 660 males.
Klinefelter syndrome doesn’t usually cause any obvious symptoms early in childhood, and even the later symptoms may be difficult to spot.
Many boys and men don’t realise they have it.
in babies and toddlers – learning to sit up, crawl, walk and talk later than usual, being weaker, quieter and more passive than usual
in childhood – shyness and low self-confidence, problems with reading, writing, spelling and paying attention, mild dyslexia and/or dyspraxia, low energy levels, difficulty socialising or expressing feelings
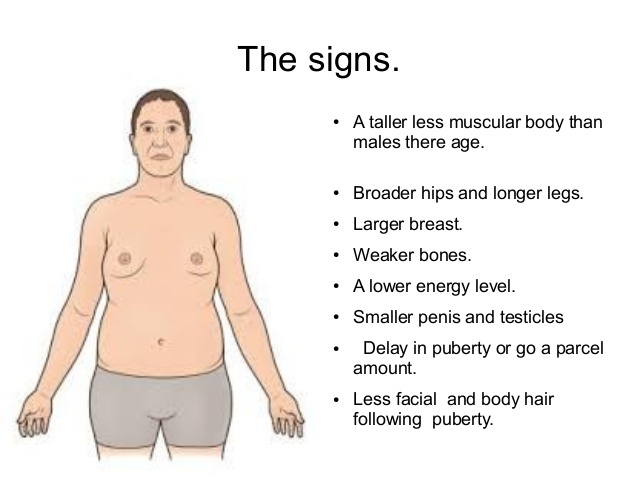
in teenagers – growing taller than expected for the family (with long arms and legs), broad hips, poor muscle tone and slower than usual muscle growth, reduced facial and body hair that starts growing later than usual, a small penis and testicles, enlarged breasts (gynaecomastia)
in adulthood – inability to have children naturally (infertility) and a low sex drive, in addition to the physical characteristics mentioned above
Most boys and men with Klinefelter syndrome will not be significantly affected and can live normal, healthy lives.
Infertility tends to be the main problem, although there are treatments that can help (see Treatments below).
However, men with Klinefelter syndrome are at a slightly increased risk of developing other health problems, including:
weak and fragile bones (osteoporosis)
cardiovascular disease and blood clots
autoimmune disorders (where the immune system mistakenly attacks the body), such as lupus
an underactive thyroid gland (hypothyroidism)
anxiety, learning difficulties and depression – although intelligence is usually unaffected
male breast cancer – although this is very rare
These problems can usually be treated if they do occur and testosterone replacement therapy may help reduce the risk of some of them.
Klinefelter syndrome is caused by an additional X chromosome.
This chromosome carries extra copies of genes, which interfere with the development of the testicles and mean they produce less testosterone (male sex hormone) than usual.
The extra genetic information may either be carried in every cell in the body or it may only affect some cells (known as mosaic Klinefelter syndrome).
Klinefelter syndrome isn’t directly inherited – the additional X chromosome occurs as a result of either the mother’s egg or the father’s sperm having the extra X chromosome (an equal chance of this happening in either), so after conception the chromosome pattern is XXY rather than XY.
This change in the egg or sperm seems to happen randomly. If you have a son with the condition, the chances of this happening again are very small.
However, the risk of a woman having a son with Klinefelter syndrome may be slightly higher if the mother is over 35 years of age.
See your GP if you have concerns about your son’s development or you notice any troubling symptoms of Klinefelter syndrome in yourself or your son.
Klinefelter syndrome isn’t necessarily anything serious, but treatment can help reduce some of the symptoms if necessary.
In many cases, it’s only detected if a man with the condition undergoes fertility tests.
Your GP may suspect Klinefelter syndrome after a physical examination and they may suggest sending off a sample of blood to check reproductive hormone levels.
The diagnosis can be confirmed by checking a sample of blood for the presence of the extra X chromosome.
There’s no cure for Klinefelter syndrome, but some of the problems associated with the condition can be treated if necessary.
Possible treatments include:
testosterone replacement therapy (see below)
speech and language therapy during childhood to help with speech development
educational and behavioural support at school to help with any learning difficulties or behaviour problems
occupational therapy to help with any co-ordination problems associated with dyspraxia
physiotherapy to help build muscle and increase strength
psychological support for any mental health issues
fertility treatment – options include artificial insemination using donor sperm or possibly intra-cytoplasmic sperm injection (ICSI), where sperm removed during a small operation are used to fertilise an egg in a laboratory
breast reduction surgery to remove excess breast tissue
TRT involves taking medication containing testosterone. It can be taken in the form of gels or tablets in teenagers, or given as gel or injections in adult men.
TRT may be considered once puberty begins and may help with the development of a deep voice, facial and body hair, an increase in muscle mass, reduction in body fat, and improvement in energy. You should see a specialist in children’s hormones (a paediatric endocrinologist) at this time.
Long-term treatment during adulthood may also help with several other problems associated with Klinefelter syndrome – including osteoporosis, low mood, reduced sex drive, low self-esteem and low energy levels – although it can’t reverse infertility.
If you or your son has been diagnosed with Klinefelter syndrome, you might find it useful to find out more about it and get in touch with others affected by it.
The following websites may be able to help:

Bell’s palsy
Bell’s palsy is a condition that causes temporary weakness or paralysis of the muscles in one side of the face. It is the most common cause of facial paralysis.
Other causes of facial paralysis include:
congenital facial palsy – children born with facial weakness
injury to the facial nerve in an accident – such as a cut to the cheek or skull base fracture
injury from surgery – which is most common during surgery of the parotid gland and neck
The symptoms of Bell’s palsy vary from person to person. The weakness on one side of the face can be described as either:
partial palsy, which is mild muscle weakness
complete palsy, which is no movement at all (paralysis) – although this is very rare
Bell’s palsy can also affect the eyelid and mouth, making it difficult to close and open them. In rare cases, it can affect both sides of a person’s face.
Read more about the symptoms of Bell’s palsy
As well as being a symptom of Bell’s palsy, facial weakness or paralysis can also be a sign of a more serious condition – such as a stroke.
Visit your nearest A&E department immediately or call 999 for an ambulance if you or someone you are with develops sudden facial paralysis, so a doctor can determine the cause.
Bell’s palsy is only diagnosed if other possible causes of your symptoms are ruled out.
Read more about diagnosing Bell’s palsy.
Bell’s palsy is believed to occur when the nerve that controls the muscles in your face becomes compressed.
The exact cause is unknown, although it’s thought to be because the facial nerve becomes inflamed, possibly due to a viral infection.
The herpes virus is thought to be the most common cause but other viruses may also be responsible.
Read more about the causes of Bell’s palsy
Bell’s palsy is a rare condition that affects about one in 5,000 people a year. It’s most common in people aged 15-60, but people outside this age group can also suffer from the condition. Both men and women are affected equally.
Bell’s palsy is more common in pregnant women and those with diabetes and HIV, for reasons that are not yet fully understood.
Around seven out of 10 people with Bell’s palsy make a complete recovery, with or without treatment.
Most people notice an improvement in their symptoms after about two to three weeks but a complete recovery can take up to nine months. The recovery time varies from person to person and will depend on the amount of nerve damage.
Prednisolone, a type of corticosteroid, is used to reduce the swelling of the facial nerve.
Eye drops may be required to prevent problems if you are unable to close your eye. Tape may also be used to close the eye while sleeping.
Read more about treatments for Bell’s palsy.
Around three in 10 people with Bell’s palsy will continue to experience weakness in their facial muscles, and two in 10 will be left with a more serious long-term problem.
Complications include:
persistent facial weakness
eye problems
difficulty with speech, eating and drinking
reduced sense of taste
facial muscle twitching
Bell’s palsy may reoccur in up to 14% of people, especially if there is a family history of the condition.
Read more about the complications of Bell’s palsy.