Autism & Aspergers. What’s the difference?
Autism & Aspergers. What’s the difference?
This video is very useful as well
Autism & Aspergers. What’s the difference?
Autism & Aspergers. What’s the difference?
This video is very useful as well

Signs That Someone Has Asperger’s from The Aspie Girl
Signs That Someone Has Asperger’s | The Aspie Girl “Hi guys! This is Alexa. In this video, I will be sharing the signs that tell you that someone might have Asperger’s. If you have any questions or requests for me, please comment them down below. Thank you for watching!”
#autism
I N S T A G R A M : https://www.instagram.com/alexa_girard/
T W I T T E R : https://twitter.com/alexa_girard98

Gary Numan talks autism, music and technology, For more on autism and technology go here.

Autism and DSM5
‘Asperger’s syndrome dropped from psychiatrists’ handbook’, is the headline in The Guardian. The news is based on a press release from the American Psychiatric Association (APA) announcing the approval by their Board of Trustees of a revised fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). The DSM was first published in 1952 and is often referred to as the ‘psychiatrists’ bible’ in the US.
The DSM is essentially designed to be a ‘user manual to diagnose mental illness’ – providing US psychiatrists with clear definitions of what pattern of symptoms correspond to specific conditions. This fifth revision, which has been a controversial issue of ongoing debate among psychiatrists and medical ethicists, is due out in May 2013.
One (amongst many) of the controversial decisions taken by the panel, made up of over 1,500 mental health experts, involved in drawing up the new draft guidelines, is to remove Asperger’s syndrome as a separate diagnosis and replace it within the term ‘autism spectrum disorder’.
In the terminology of the DSM-5 – Asperger’s syndrome would be seen as being at the ‘upper end’ of the autistic spectrum disorder (ASD). That means people with this type of ASD would normally have unaffected intelligence and language development, but would have milder symptoms affecting social interaction, behaviour and language comprehension.
A message about DSM-5 written by the president of the APA (PDF, 105Kb), Dr Dilip Jeste, touches on the complexities and challenges of revising an established diagnostic system, as reported in the media. These include conflicting views among experts and the under-diagnosis and over-diagnosis of patients.
Dr Jeste also says that narrowing diagnostic criteria is often blamed for excluding some patients from insurance coverage in the US, yet efforts to diagnose more patients are sometimes criticised for expanding the market for the pharmaceutical industry.
The chair of the taskforce responsible for overseeing the DSM-5 revisions, Dr David Kupfer, said: ‘Our work has been aimed at more accurately defining mental disorders that have a real impact on people’s lives, not expanding the scope of psychiatry’.
Despite the media hype, the revised classifications in DSM-5 will have limited impact on individuals who receive mental health care in the UK, at least in the short-term.
Psychiatrists in the UK tend to use the World Health Organisation’s International Classification of Diseases (ICD) system to diagnose mental health conditions, rather than DSM, which is used in the US.
Also, the term ‘autistic spectrum disorder’ (and the concepts underpinning it) have been widely used in the UK for many years. However, in the long-term, it is difficult to predict the potential impact the DSM-5 will have on the future diagnosis and treatment of mental health conditions.
Earlier versions of the DSM have had considerable influence, both in the US and across the world, in shaping opinions and driving research agendas. For example, it was the publication of the previous version (DSM-4) in 1994 that helped ‘popularise’ attention deficit hyperactivity disorder.
The DSM-5 (the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders) is produced by the American Psychiatric Association (APA) and is the diagnostic manual used by US clinicians and researchers to diagnose and classify mental disorders. The Diagnostic and Statistical Manual (DSM), first published in 1952, has undergone several revisions to take into account progress in medical and scientific knowledge and an advanced understanding of mental illnesses.
The DSM-5 is set for publication in May 2013 and will be a revision of the DSM-4 that was produced nearly 20 years ago.
According to a message from APA President, Dr Jeste, the DSM-5 reflects the best scientific understanding of psychiatric disorders and will optimally serve clinical and public health needs. Dr Jeste says ‘the hope is that the DSM-5 will lead to more accurate diagnoses, better access to mental health services, and improved patient outcomes.’
The DSM is broadly based on the classification system published by the World Health Organization (WHO), called the International Classification of Diseases (ICD).
The ICD system is used by the UK and other members of the WHO. It allows doctors to look at clusters of symptoms to form diagnoses for all health-related conditions, including mental health conditions.
The current version is ICD-10, and it is ICD-10, rather than DSM, that psychiatrists in the UK predominantly use to diagnose mental health conditions.
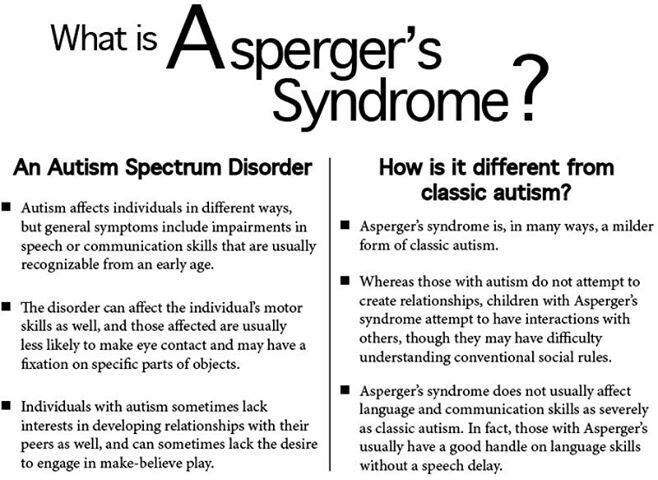
Autism and Asperger’s syndrome are both part of a range of related developmental disorders, which are characterised by:
The main difference between autism and Asperger’s is that people with ‘classic autism’ tend to have some degree of intellectual impairment. According to the press release, several categories from DSM-4 (including Asperger’s syndrome) will be replaced by a single diagnostic category of autism spectrum disorders in DSM-5. The following disorders will be incorporated under the diagnosis of autism spectrum disorders:
autistic disorder
Asperger’s syndrome
childhood disintegrative disorder
pervasive developmental disorder (not otherwise specified)
The press release says that this is to help more accurately and consistently diagnose people with autism. This does not mean that Asperger’s syndrome is being removed from the DSM classification system, only that it is being placed under a single diagnostic category.
Under ICD-10, both autism and Asperger’s syndrome are classed under what are known as ‘pervasive developmental disorders’ – pervasive meaning that the characteristic features of these conditions (for example, social interaction and communication problems) are a feature of the person’s functioning in all life situations.
According to the press release, the DSM-5 will include approximately the same number of disorders that were included in the DSM-4.
Additional mental disorders set to be included in the DSM-5 are:
disruptive mood dysregulation disorder – which is intended to address concerns about potential over diagnoses and overtreatment of bipolar disorder in children
excoriation (skin picking) disorder – which will be included in the obsessive-compulsive and related disorders section
hoarding disorder – which is said to be supported by extensive scientific research on this disorder and included to help characterise people with persistent difficulty discarding or parting with possessions regardless of their actual value
The revised manual (DSM-5) will include a section on conditions that require further research before their consideration as formal disorders. This section will include:
attenuated psychosis syndrome – where people have psychotic-like symptoms (such as hearing voices), but not full-blown psychosis (unable to tell the difference between reality and their imagination)
internet use gaming disorder – essentially, an online gaming addiction
non-suicidal self-injury – self-harming behaviour, but not with the intent of ending life
suicidal behavioural disorder – a type of personality disorder that increases the risk of a person taking their own life
Disorders that will not be included in the revised manual (DSM-5) include:
anxious depression – a term proposed to describe mild to moderate symptoms of anxiety and depression
hypersexual disorder – so called ‘sex addiction’. For more information see our October 2012 analysis “Media claims ‘sex addiction is real“.
parental alienation syndrome – a term proposed to describe a child who ‘on an ongoing basis, belittles and insults one parent without justification’
sensory processing disorder – a term proposed to describe people who have difficulties processing sensory information (for example, visual information or sounds)
Other changes to the DSM-5 reported in the press release include:
a broadening of the criteria for specific learning disorders
a new chapter on post-traumatic stress disorder that will include information for children and adolescents
removal of certain bereavement exclusion criteria – making clearer the difference between natural feelings of grief and mental illness.
Until the publication of the DSM-5 in May 2013, there will be no changes to diagnoses of mental disorders. Importantly, the DSM-5 is a US publication, so its main impact will be in the US where clinicians use the DSM-5 to diagnose mental disorders.
Clinicians in the UK predominantly use the ICD-10 system to diagnose mental disorders, while the DSM classification system is mostly used for research purposes.
As mentioned, in the long-term, the new version of the DSM may have long-term healthcare, as well as cultural and political, implications that are impossible to predict.

Parent-mediated social communication
“A new form of therapy has for the first time been shown to improve the symptoms and behaviour of autistic children,” The Guardian reports.
A new trial looked at the impact of early intervention in children with severe autism. This programme of treatment aimed to mainly focus on the parents, who were trained to pick up on communication cues from their child, which are usually much more subtle than in other children.
For example, a small shift in head movement could be a sign that the child wanted to communicate.
The hope is that once parents receive sufficient training they can then provide “around the clock” therapy to their child rather than one-off sessions provided by external therapy.
The programme, Parent-mediated social communication therapy for young children with autism (known as PACT), showed early promise. The children of parents who took the course showed improvements in symptoms such as communication and repetitive behaviour after one year. This study tested the children again, five to six years after the end of treatment, to see if the effects had lasted.
The children in the PACT group had on average lower symptoms scores for autism when compared to those who had normal care. But the difference was small enough that it could have been down to chance (it wasn’t statistically significant). That doesn’t mean the treatment didn’t work, but arguably suggests the PACT programme should be now tested in larger groups of families affected by autism.
The study was carried out by researchers from Kings College London, Newcastle University, the University of Manchester and Guys and St Thomas University NHS Trust and was funded by the Medical Research Council, Department of Health and National Institute of Health Research.
The study was published in the peer-reviewed journal The Lancet on an open-access basis, so it’s free to read online.
Most of the UK media reports were enthusiastic. The Daily Telegraph called it “the first successful treatment for autism” while The Guardian reported a “potential breakthrough”.
But at the risk of sounding like a kill-joy, none of the media sources mentioned that the main finding of the study was not statistically significant.
Many made the effort to include some useful feedback and commentary from independent experts. For example, Dr James Cusack, the director of science at the charity Autistica, was quoted widely, saying: “Too often, parents fall victim to the false claims of charlatans who prey on desperate families.
“These results look promising for the many thousands of parents who want to find early interventions for their children based on solid science,”
This was a long-term follow up of a randomised controlled trial. These types of studies are usually good ways to assess the effects of treatments.
Researchers randomly divided parents of pre-school children with autism into two groups.
One group of 75 had normal care, while in the other group, 77 parents were coached in how to communicate better with their children, using videos of play sessions to spot opportunities for communication.
The programme, called PACT, lasted for a year.
Five to six years later, researchers contacted the families again and asked them to have follow-up tests of autism symptoms.
They compared the results from the group who’d had normal care with those who’d had PACT.
In the PACT training, parents were coached to recognise what might be very subtle clues that their children wanted to engage with them and then respond appropriately, in a way that was intended to help children learn social interaction and language.
They had 12 two-hour coaching sessions over six months, then a further six support sessions over six months.
Unlike many treatments for autism, therapists worked with the parents rather than directly with the children. The aim was to produce long-lasting improvements, by changing the children’s home environment.
Children were aged between two and four years 11 months when they started in the study. The average age at follow-up was 10 and a half.
Follow up assessments for the main results were done by researchers who didn’t know which treatment group the children had been in.
The researchers also asked parents about their children’s symptoms and behaviour.
They analysed the data in different ways, but the main result was a change in autism symptom score severity.
They looked at children’s scores at the start of the study, after the 12 month treatment period, and at follow up.
The original study showed that children in the PACT group had a bigger improvement in symptom scores after treatment, compared to those who’d had usual care.
At follow-up, both groups of children had worse scores than immediately after the study.
There was still a difference between the groups, but it was no longer statistically significant.
That means we cannot be sure that, five years on from treatment, PACT improved average symptom scores more than normal care.
Average scores (1 to 10, higher being more severe) were:
8.0 for PACT and 7.9 for usual care at the start of the study
6.7 for PACT and 7.3 for usual care immediately after the study
7.3 for PACT and 7.8 for usual care at follow-up
Fewer children in the PACT group had severe symptom scores at follow up (46%) than those who’d had usual care (63%).
The difference between the groups was too small to be sure this was not simply a chance finding (group difference 17.2%, 95% confidence interval [CI] -2.9 to 37.3).
However, looking at the combined mean symptoms scores from immediately after the study and at follow-up compared to baseline (before treatment), the results show a statistically-significant moderate effect in favour of PACT treatment (effect size 0.55, 95% CI 0.14 to 0.91).
The researchers say their results “are encouraging and provide evidence that sustained changes in autism symptoms can be possible after early intervention,” in a way that has not been shown before.
They go on to say that “on the basis of these results, we are now able to support the use of the PACT intervention for reducing symptoms of autism in young children”.
They caution that the treatment has not yet been tested in older children, or in children with autism spectrum disorder, rather than “core” autism.
This study seems to provide some much-needed good news for parents of children with autism, and has been welcomed by experts and campaigners. However, the lack of statistical significance of some of the results mean we can’t be sure the findings are reliable.
Statistical significance is a way of including a margin of error in calculations and allowing for chance. So the “true result” for PACT could be between 6.3 and 8.3, and the true results for usual care could be between 6.9 and 9.6. As these results overlap, we can’t be sure that PACT treatment led to better scores.
One expert said that the main outcome measure of the autism symptom scale is “insensitive to change” meaning that it may not be the best way to show improvements. Another said the effects of PACT in the study were “not dramatic” and “very variable” across the group of children.
However, most seem to think that the results are promising, especially for an intervention that does not require the intensive time and commitment of some other autism treatments.
The National Institute for Health and Care Excellence says “social communication interventions” should be considered for children with autism, although it doesn’t mention PACT specifically.
Hopefully further trials of PACT in larger groups of parents will point to a significant improvement in autism symptoms.