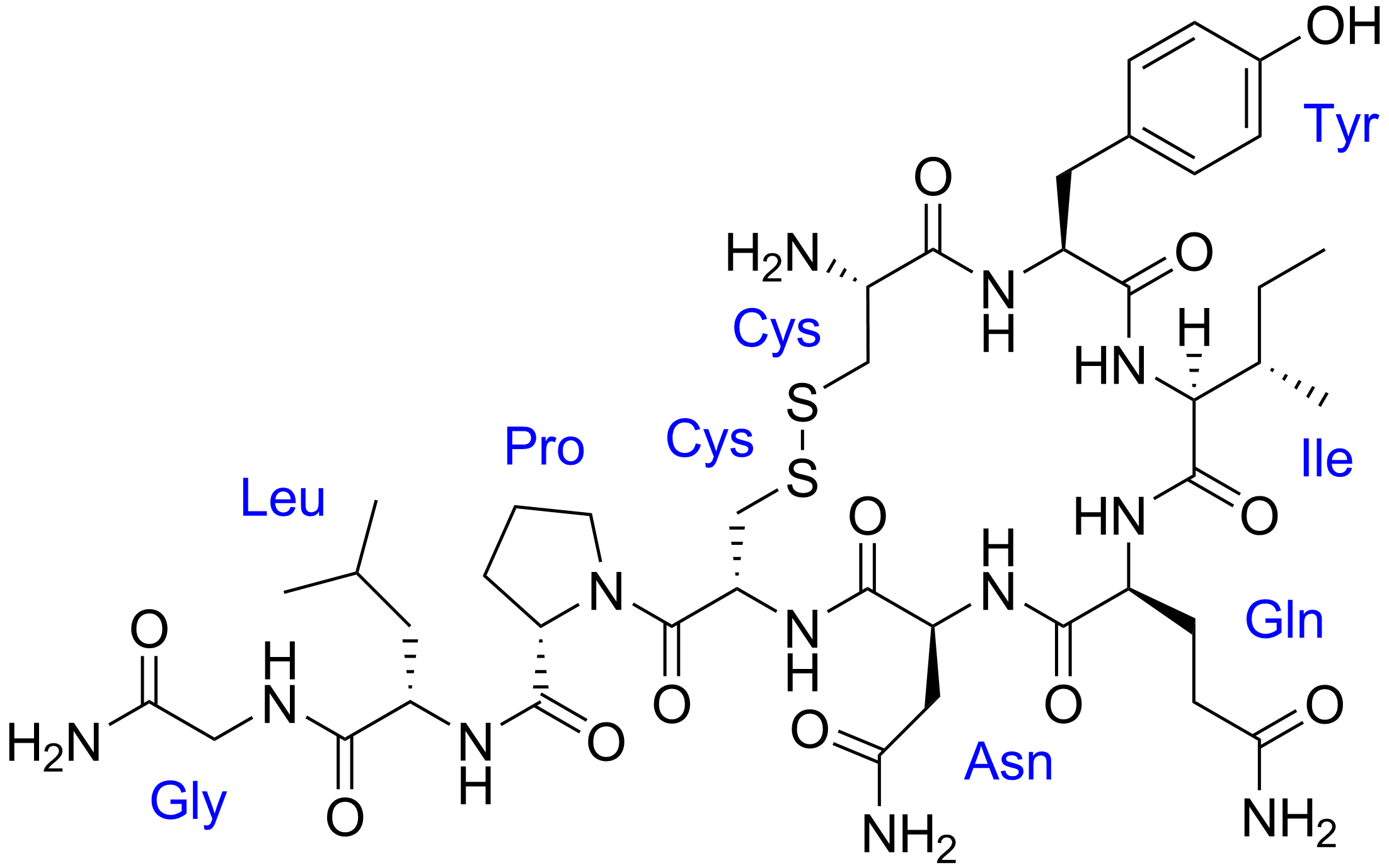
Oxytocin, a naturally occurring hormone that acts as a chemical messenger in the brain, showed no evidence of helping children with autism gain social skills, according to a large national study appearing Oct. 13 in the New England Journal of Medicine.
While disappointing for those holding hope that oxytocin could benefit children with autism, the long-awaited finding provides clarity for a drug that has shown mixed outcomes in smaller, less robust studies.
“There was a great deal of hope this drug would be effective,” said the study’s principal investigator and lead author, Linmarie Sikich, M.D., associate consulting professor in the Department of Psychiatry & Behavioral Sciences at Duke University School of Medicine. “All of us on the study team were hugely disappointed, but oxytocin does not appear to change social function of people with autism.”
Oxytocin is typically used to induce labor, but because of its activity in the brain, it has been investigated as a treatment for autism. Evidence has been conflicting, with several smaller studies suggesting it improved social and cognitive function among some children with autism, while other studies showed no benefit.
Sikich and colleagues, including senior author Jeremy Veenstra-VanderWeele, M.D., of New York State Psychiatric Institute and Columbia University, designed the multi-site trial to provide the best evidence yet about whether oxytocin was a safe and effective treatment for children with Autism.
The research team enrolled 290 children ages 3-17, stratified by age and the severity of their autism symptoms. The children were randomized in similar, equal-sized groups to receive oxytocin or a placebo via a daily nasal spray over 24 weeks.
The study aimed to see if the regimen of oxytocin would have a measurable impact on the children’s social abilities based on screenings and assessments at the start of the trial, midway through and at the end. Both researchers and the children’s parents provided assessments using standard analytic tools for autism.
While the oxytocin was well tolerated and had few side effects, it showed no significant benefit among the group of children who received it compared to those who received the placebo.
“Thousands of children with autism spectrum disorder were prescribed intranasal oxytocin before it was adequately tested,” Veenstra-VanderWeele said. “Thankfully, our data show that it is safe. Unfortunately, it is no better than placebo when used daily for months. These results indicate that clinicians and families should insist that there is strong evidence for the safety and benefit of new treatments before they are provided to patients in the clinic.”
Sikich said no further study is likely of oxytocin, given the negative findings: “Our consensus as investigators is that there is no evidence in this large study that is strong enough to justify more investigation of oxytocin as a treatment for autism spectrum disorders.”
Many variants in the human genome have been linked to type 2 diabetes, but because most do not lie within genes that code for proteins, it’s unclear how they might cause disease. Now an international team, including investigators at Massachusetts General Hospital (MGH), has developed a resource to help uncover the impact of these genetic variants.
The work, which is described in Cell Reports, relies on the knolwedge that abnormalities in groups of pancreatic cells called islets, which produce and release hormones that regulate blood sugar levels, drive the development of type 2 diabetes. Unfortunately, however, it’s very difficult to obtain samples of human islets. To overcome this challenge, scientists from Spain, Belgium, Italy, Sweden, Finland, the UK, and the US banded together to obtain more than 500 human islet samples from patients with and without type 2 diabetes and to extract genomic and gene expression data from these samples. With these data, the researchers created what they named TIGER (for Translational human pancreatic Islet Genotype tissue-Expression Resource).
The research required collecting and examining an enormous amount of information, which was made possible through the use of supercomputing resources and new statistical methods.
Analyses of TIGER revealed that certain genetic variants in islets from patients with type 2 diabetes control the expression of particular genes. So far, 32 novel genes were identified that may contribute to type 2 diabetes risk.
“This resource will be very useful to identify genes that may be related with the genetic variants that we have found associated with type 2 diabetes,” says co–senior author Josep M. Mercader, PhD, a research-scientist at MGH’s Diabetes Unit and Center for Genomic Medicine. “Knowing the gene behind a given genetic association is the first step for identifying potential drug targets, or to better understand the physiology of different types of diabetes.”
TIGER’s data are publicly available and easily accessible to the diabetes research community through the TIGER web portal (tiger.bsc.es).
“We are proud that we are now able to share this wealth of data to the scientific community in an easily accessible way for all researchers in the type 2 diabetes field, without the need of computational or bioinformatic expertise,” says co–lead author Lorena Alonso, of the Barcelona Supercomputing Center, in Spain, one of the developers of the TIGER portal.
Co–lead authors include Ignasi Moran, PhD, of the Barcelona Supercomputing Center and Anthony Piron, of the Université Libre de Bruxelles. Co–senior authors include Miriam Cnop, MD PhD, of the Université Libre de Bruxelles, and David Torrents, PhD, of the Barcelona Supercomputing Center.
Intermittent fasting can produce clinically significant weight loss as well as improve metabolic health in individuals with obesity, according to a new study review led by University of Illinois Chicago researchers.
“We noted that intermittent fasting is not better than regular dieting; both produce the same amount of weight loss and similar changes in blood pressure, cholesterol and inflammation,” said Krista Varady, professor of nutrition at the UIC College of Applied Health Sciences and author of “Cardiometabolic Benefits of Intermittent Fasting.”
According to the analysis published in the Annual Review of Nutrition, all forms of fasting reviewed produced mild to moderate weight loss, 1%-8% from baseline weight, which represents results that are similar to that of more traditional, calorie-restrictive diets. Intermittent fasting regimens may also benefit health by decreasing blood pressure and insulin resistance, and in some cases, cholesterol and triglyceride levels are also lowered. Other health benefits, such as improved appetite regulation and positive changes in the gut microbiome, have also been demonstrated.
The review looked at over 25 research studies involving three types of intermittent fasting:
Alternate day fasting, which typically involves a feast day alternated with a fast day where 500 calories are consumed in one meal.
5:2 diet, a modified version of alternate day fasting that involves five feast days and two fast days per week.
Time-restricted eating, which confines eating to a specified number of hours per day, usually four to 10 hours, with no calorie restrictions during the eating period.
Various studies of time-restricted eating show participants with obesity losing an average of 3% of their body weight, regardless of the time of the eating window.
Studies showed alternate day fasting resulted in weight loss of 3%-8% of body weight over three to eight weeks, with results peaking at 12 weeks. Individuals on alternate day fasting typically do not overeat or binge on feast days, which results in mild to moderate weight loss, according to the review.
Studies for the 5:2 diet showed similar results to alternate day fasting, which surprised the study’s reviewers. The subjects who participate in the 5:2 diet fast much less frequently than alternate-day fasting participants do, but the results of weight loss results are similar.
Weight loss in both the alternate day and 5:2 fasting are comparable to more traditional daily calorie-restrictive diets. And, both fasting diets showed individuals were able to maintain an average of 7% weight loss for a year.
“You’re fooling your body into eating a little bit less and that’s why people are losing weight,” Varady said.
Varady added the review set out to debunk some myths regarding intermittent fasting. Intermittent fasting does not negatively affect metabolism, nor does it cause disordered eating, according to the studies reviewed.
“Fasting people are worried about feeling lethargic and not being able to concentrate. Even though you are not eating, it won’t affect your energy,” Varady said. “A lot of people experience a boost of energy on fasting days. Don’t worry, you won’t feel crappy. You may even feel better.”
The study review includes a summary of practical considerations for those who may want to try intermittent fasting. Among the considerations are:
Adjustment time — Side effects such as headaches, dizziness and constipation subside after one to two weeks of fasting. Increased water intake can help alleviate headaches caused by dehydration during this time.
Exercise — Moderate to high-intensity endurance or resistance training during food abstention can be done, and some study participants reported having more energy on fast days. However, studies recommend those following alternate day fasting eat their fasting day meal after exercise.
Diet during fasting — There are no specific recommendations for food consumption during intermittent fasting, but eating fruits, vegetables and whole grains can help boost fiber intake and help relieve constipation that sometimes accompanies fasting.
Alcohol and caffeine — For those using an alternate day or 5:2 fasting plan, alcohol is not recommended on fast days as the limited calories should be used on healthy foods that provide nutrition.
There are several groups who should not intermittent fast, according to the studies. Those individuals include:
Those who are pregnant or lactating.
Children under 12.
Those with a history of disordered eating.
Those with a body mass index, or BMI, less than 18.5.
Shift workers. Studies have shown they may struggle with fasting regimens because of shifting work schedules.
Those who need to take medication with food at regimented times.
“People love intermittent fasting because it’s easy. People need to find diets that they can stick to long term. It’s definitely effective for weight loss and it’s gained popularity because there are no special foods or apps necessary. You can also combine it with other diets, like Keto,” Varady said.
Mindful breathing for pain control: Like yin and yang
It’s long been known that meditative mindful breathing helps with various health conditions, including pain.
To that end, researchers at the University of Michigan compared two types of meditative breathing––traditional mindful breathing and virtual reality, 3D-guided mindful breathing––to reduce pain. They found that each lessened pain by modulating the somatosensory cortex, a region of the brain responsible for processing pain, but each used different mechanisms, said Alexandre DaSilva, associate professor at the School of Dentistry.
With the traditional breathing group, the functional connection with the brain’s frontal regions increased, because this region was focused on the body’s internal sensory details, called interoception, DaSilva said. This competed with the external pain signals and inhibited the ability of the somatosensory cortex to process pain. This follows the common assumption that mindful breathing exerts its painkilling effect by interoception, which means the conscious refocusing of the mind’s attention to the physical sensation of an internal organ function.
In the virtual reality group, subjects wore special glasses and watched a pair of virtual reality 3D lungs, while breathing mindfully. The technology was developed in-house and the lungs synchronized with the subjects’ breathing cycles in real time. This provided an immersive visual and audio external stimulus. Pain decreased when the sensory regions of the brain (visual, auditory) engaged with the immersive virtual reality sound and image stimulations. This is called exteroception, and it weakened the pain processing function of the somatosensory cortex.
“(I was surprised) that both meditative breathing methods decreased pain sensitivity, but oppositely in the brain, like yin and yang,” DaSilva said. “One by engaging the brain in an immersive exterior 3D experience of our own breathing, or exteroception––yang, and the other by focusing on our interior world, interoception––yin.”
Though both approaches decreased pain sensitivity, traditional mindful breathing can be challenging because it requires long-time attention and focus on an abstract experience, he said. Virtual reality breathing might be more accessible, especially for beginners, because it lends an immersive “visual and auditory guide” to the meditation experience.
And, the virtual reality mindful breathing gives medical professionals another possible option for pain relief, to decrease the tendency to rely solely on pain medications, including opiates, DaSilva said.
Pain is processed by many regions in the brain that provide different information for the global pain experience. DaSilva’s lab learned in previous studies that some of those regions can be externally targeted by neuromodulation, a process whereby electrical impulses are used to directly modulate brain activity.
However, here was to dissect and understand the two brain mechanisms for pain modulation using breathing. To that end, DaSilva’s team compared the two methods of breathing, by placing a single, unilateral thermode on the left mandibular nerve branch of the trigeminal cranial nerve for each participant––think of a tiny, computer-controlled hotplate on your face.
To study the brain mechanisms used during the two types of breathing, researchers analyzed their associated functional connectivity––i.e., what regions of the brain were co-activated and when––during each type of breathing and pain stimulation. They investigated the acute (same session) and long effects (after one week) of breathing techniques, and in the week between the two neuroimaging sessions, both groups did traditional mindful breathing at home.
DaSilva’s research group, which focuses heavily on migraine and pain, is working on options to deliver this virtual reality breathing experience via a mobile application and extending its clinical benefit to multiple chronic pain disorders beyond the lab space.
Researchers at the University of Chicago have developed a novel computational approach that can reliably predict an eventual diagnosis of autism spectrum disorder (ASD) in young children, without the need for additional blood work or procedures, using only diagnostic codes from past doctor’s visits. The new approach reportedly reduces the number of false positive ASD diagnoses produced by traditional screening methods by half.
ASD can be diagnosed as early as age 2, but false positives flagged by the initial screens traditionally used today can delay the confirmation of a true diagnosis. Given the value of early intervention and the limited number of trained professionals, tools that can potentially reduce the pool of patients required to undergo the lengthy, multistep process to receive an official positive diagnosis can have a profound impact on patient care.
Traditionally, questionnaire-based screening tools are used as the first step in identification of ASD. “But, these are prone to inaccuracies that may arise due to things such as a language barrier or culture barrier, and can give rise to inaccurate diagnoses. By only looking at the data as objectively as possible, our approach avoids some of the pitfalls of traditional screening approaches,” said lead author Dmytro Onishchenko, a senior scientist in the Zero Knowledge Discovery (ZeD) Lab led by Ishanu Chattopadhyay, PhD, Professor of Medicine.
The study, a collaboration between the ZeD Lab and University of Chicago developmental pediatricians Dr. Michael E. Msall, MD, and Dr. Peter J. Smith, MD, was published on October 6 in Science Advances.
Using only sequences of ICD9 and ICD10 (International Classification of Diseases) diagnostic codes generated from past doctor’s visits, which are available for any consenting patient, the researchers were able to leverage known comorbidities of ASD to reliably predict an eventual positive diagnosis.
“Using the information already being gathered and being able to harness it for this kind of exploration and clinical use is exciting, and it really has the potential to be a game changer,” said Smith.
The researchers’ new algorithm determines an autism comorbid risk score (ACoR), which estimates the risk that a child with a given timeline of diagnoses will eventually receive a confirmed ASD diagnosis. The research applied advances in medical informatics to over 30 million de-identified diagnostic sequences representing over 15,000 distinct ICD codes, originating from the Truven Health Analytics and University of Chicago Medical Center (UCM) databases. The team separated these profiles into positive (i.e., an official ASD diagnosis) and controls. They then applied algorithms that “learned” patterns representative of ASD-positive cohorts compared to ASD-negative cohorts. This research strategy allowed them to find which disease categories contribute to the ACoR and how much each category contributes.
When these risk scores are calculated for an individual patient, the researchers can quantify how far their unique diagnostic timeline deviates from either the positive or control group. When that risk score crosses a threshold, a patient can be flagged as possibly requiring interventions.
By several standard metrics, ACoR outperformed the commonly used questionnaire-based M-CHAT/F screening method, as well as other methods that have made use of comorbidity patterns, including a higher probability that a flagged patient will receive a confirmed ASD diagnosis. Importantly, the researchers were able to flag patients as at-risk more than one year earlier than their actual diagnosis.
Importantly, ACoR performed consistently well for different racial and ethnic groups and even in U.S. counties where diagnostic resources are scarce. “A lot of what we have done is take the data and processes available in better connected systems and apply them to less well supported healthcare communities. We know for instance that African American individuals are frequently diagnosed later, which has an impact on long term care. This type of technology could overcome some of these structural barriers,” said Smith.
None of this should be taken to mean that the old paradigm for autism screening should be thrown out. Despite their exciting results, the researchers see this new tool as complementary to methods like M-CHAT/F.
“Many machine learning-based approaches, particularly those trying to do autism screening, may aim to replace or mimic the physician. But people like Dr. Msall and Dr. Smith have been doing this for many years. Maybe someday machine learning will be able to replace human decision making, but we are not there yet,” said Chattopadhyay. “The point of this approach is to leverage underutilized modalities, to do computations that the human brain cannot, to complement the physician.”
In addition, Msall said, “Our goal is to perform enablement diagnostic confirmation and help families access the pathways that promote on-going communicative, social and adaptive learning during times of maximum neuroplasticity.”
In fact, when used in tandem with the screening results from M-CHAT/F, ACoR performs even better. There is no substitute for the expertise of a trained specialist or the careful observation of parents, but when 85% of the patients flagged by M-CHAT/F are false positives, objective, data-driven approaches like ACoR, which can be administered even without the patient being present, can fill in the gaps sometimes created by the subjectivity of other measures. The ZeD lab hopes to see their tool widely adopted so that it can reduce the number of false positive patients, who would still need to undergo subsequent screening, and cut down the waiting times for families seeking care for their children.
“Our paradigm shift is more than appropriate early identification. Our paradigm shift is engagement, community flexibility, and recognition of neurodiversity,” said Msall. “Autism is an epidemic, but children can still thrive with this diagnosis. We can bring systematic population-level science, data science, and decision-making science together so that we can appropriately support the families in new and creative ways.”
The study, “Reduced false positives in autism screening via digital biomarkers inferred from deep comorbidity patterns”, was supported by the Defense Advanced Research Projects Agency (DARPA) project number HR00111890043/P00004 . Additional authors include Yi Huang and James van Horne, both of the University of Chicago.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.