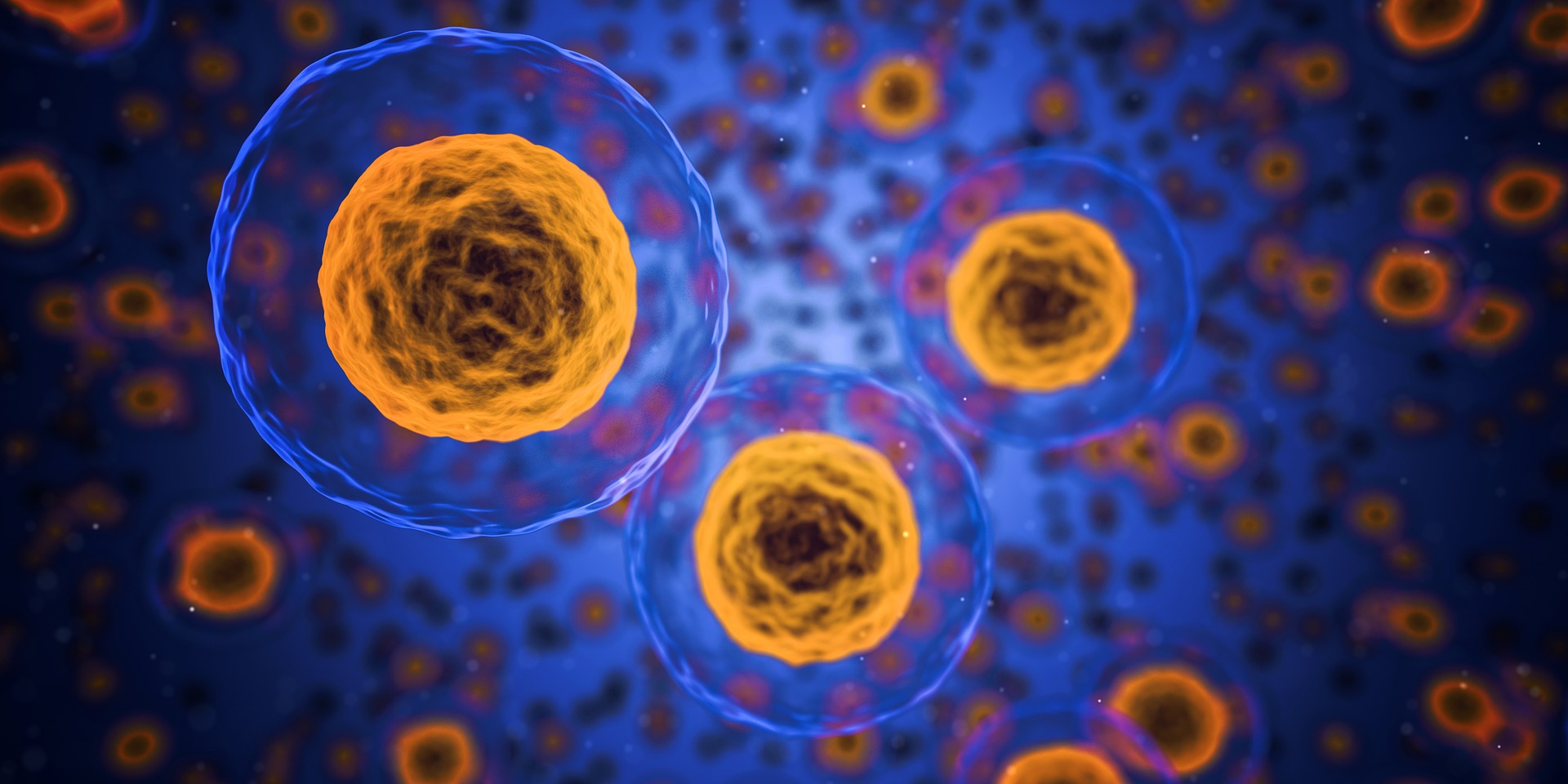
Immunofluorescent images of kidney tissue show inflammation in green. The kidney tissue shown on the right was treated with an NKp46 receptor-blocking antibody, resulting in significantly reduced inflammation. Credit Charité
A team led by Charité – Universitätsmedizin Berlin, the German Rheumatology Research Center, and the Max Delbrück Center has identified key cells responsible for severe kidney damage in lupus. The research, which was published in “Nature,” can provide valuable insights for future antibody therapies.
A research team in Berlin has discovered key regulators of severe kidney damage in patients with lupus, an autoimmune disorder that affects an estimated five million people worldwide, most of whom are young women. They found that a small, specialized population of immune cells known as innate lymphoid cells (ILCs) triggers a cascade of effects that lead to harmful kidney inflammation, also known as lupus nephritis.
The research published this week in “Nature” challenges the traditional belief that autoantibodies, which are proteins produced by immune cells and mistakenly attack healthy tissues, are the primary cause of lupus nephritis.
“Autoantibodies alone are not enough to cause tissue damage. Our research shows that ILCs (innate lymphoid cells) play a crucial role in amplifying the damage to organs,” explained Dr. Masatoshi Kanda, a senior author of the study. Dr. Kanda was a Humboldt Fellow at Max Delbrück Center and is currently based at the Department of Rheumatology and Clinical Immunology at Sapporo Medical University in Japan.
Lupus, also known as systemic lupus erythematosus, is typically diagnosed between the ages of 15 and 45. The symptoms can vary in severity from mild to severe. However, the reason behind kidney damage in certain patients, to the extent of needing dialysis, has remained unclear.
“We have now identified most of the circuit controlled by ILCs in lupus nephritis by examining the entire kidney at single-cell resolution,” says Professor Antigoni Triantafyllopoulou of the German Rheumatology Research Center.
Unusual immune cells
ILCs are a small group of immune cells that live in a specific tissue or organ, unlike most other immune cells that circulate throughout the body.
“They are present in the tissues all the time, starting from the embryonic development stage, which sets them apart from other immune cells,” stated Professor Andreas Diefenbach, a senior author of the paper and the director of the Institute of Microbiology, Infectious Diseases, and Immunology at Charité – Universitätsmedizin Berlin.
Diefenbach’s laboratory was one of the first to discover ILCs in the mid-2000s. Most of his research is focused on ILCs in the gut and their effects on tissue function. In this study, Triantafyllopoulou and Kanda collaborated with Diefenbach’s group and Dr. Mir-Farzin Mashreghi at the DRFZ to investigate the presence of ILCs in the kidney and their potential role in lupus nephritis.
The whole single-cell picture
To unravel this mystery, the team utilized single-cell RNA sequencing, which identifies active genes in individual cells, helping researchers understand the cells’ identity and function.
Kanda, a rheumatologist who was studying bioinformatics in Professor Norbert Hübner’s lab at the Max Delbrück Center at the time, developed a specialized protocol for single-cell RNA sequencing of mouse and human kidneys. “Masatoshi’s protocol was very good at pulling out and preserving multiple types of kidney cells, which gave us a much more complete overview of how lupus affects the whole kidney,” explains Triantafyllopoulou. The team sequenced nearly 100,000 individual kidney and immune cells of various types and functions.
The key receptor
The research team found that a specific group of ILCs, which have a receptor called NKp46, play a key role in causing lupus nephritis in mice. When NKp46 is activated, these cells increase their production of a protein called GM-CSF, which in turn stimulates invading macrophages to multiply. Macrophages are large immune cells that consume dying cells and microbes. In the kidney, the influx of macrophages leads to severe tissue damage and the accumulation of scar tissue, known as fibrosis.
“These ILCs are really amplifiers in this system,” Diefenbach says. “They are small in population, but they seem to fertilize the whole process.”
When the team blocked NKp46 with antibodies or genetically removed the receptor, kidney tissue damage was minimal. They also blocked GM-CSF, which had similar anti-inflammatory effects.
“Critically, autoantibody levels did not change when NKp46 was inhibited, but kidney tissue damage was reduced, which shows autoantibodies are not directly responsible for kidney inflammation,” Triantafyllopoulou explains.
The research team also compared the results to sequencing data from tissue taken from human patients with lupus. They found that ILCs were present, but they stated that more work is needed to fully understand how to target ILCs in human kidneys. However, the detailed studies provided new insights that suggest potential antibody therapies for patients with severe forms of lupus. The ultimate goal is to prevent the need for kidney dialysis in these patients.