This is a great introduction to Williams syndrome you can share with your friends and family.
Y
Williams Syndrome Awareness from Williams Syndrome Association on Vimeo.
This is a great introduction to Williams syndrome you can share with your friends and family.
Y
Williams Syndrome Awareness from Williams Syndrome Association on Vimeo.
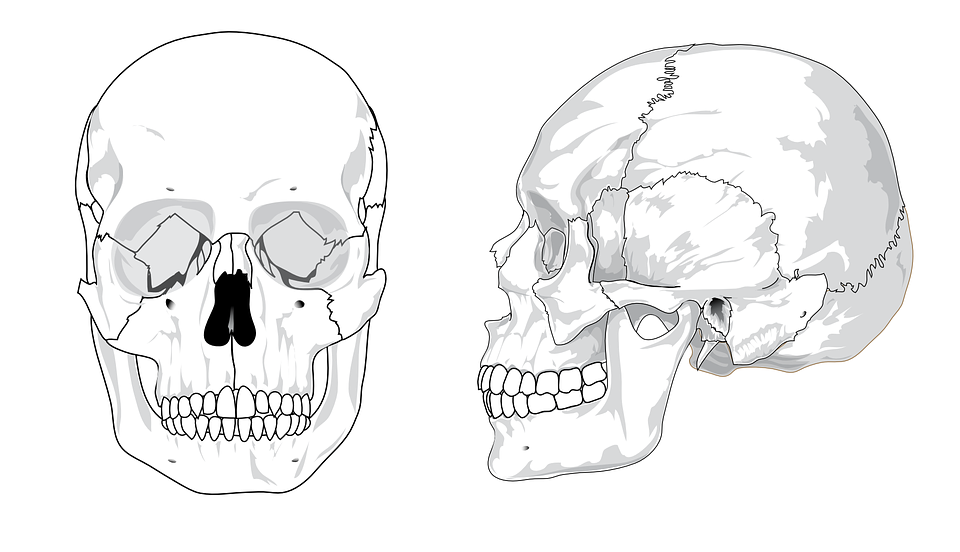
Craniosynostosis
Craniosynostosis causes an irregular skull shape. The baby’s skull shape is determined by the type of craniosynostosis they have.
A baby’s skull consists of seven plates of bone connected by strong elastic tissues called sutures. The sutures give the bone plates flexibility so the skull can grow along with the brain.
Other signs of craniosynostosis can include:
a hard ridge developing along the sutures
the soft spot (fontanelle) on your baby’s head disappearing or feeling different
your baby’s head not growing in proportion with the rest of their body
an increase in pressure within the baby’s skull or raised intracranial pressure (ICP)
In some cases, craniosynostosis may not be noticeable until a few months after birth.
Raised intracranial pressure (ICP) is a symptom that may occur in all types of craniosynostosis. ICP increases when pressure builds up inside your child’s skull because of its irregular shape.
When only one suture is involved, raised ICP occurs in less than 15% of children. However, in syndromic craniosynostosis where multiple sutures are involved, raised ICP is more common and may occur in up to 60% of cases.
If your child has mild craniosynostosis, it may not be spotted until they begin to experience problems because of an increase in ICP. This usually occurs when a child is between four and eight years old.
The symptoms of ICP usually begin with:
a persistent headache – usually worse in the morning and last thing at night
vision problems – such as double vision, blurred vision, or a “greying out” of vision
an unexplained decline in the child’s academic abilities
If your child complains of any of the above symptoms, take them to see your GP as soon as possible. In most cases, these symptoms will not be caused by raised ICP, but they do require further investigation.
Left untreated, other symptoms of raised ICP can include:
vomiting
irritability
sluggishness and unresponsiveness
swollen eyes or difficulty following a moving object
hearing difficulties
breathing difficulties
There are several types of craniosynostosis, depending on which sutures are affected. Different sutures being affected can lead to a different shaped skull.
These are described below.
Sagittal synostosis is the most common type of craniosynostosis, accounting for around half of all cases.
It occurs when the suture at the top of the skull (the sagittal suture) fuses. This leads to a lack of growth in width and compensatory growth in length, resulting in a long, narrow skull.
Coronal craniosynostosis is the second most common type of craniosynostosis after sagittal synostosis, accounting for around one in four cases.
In coronal craniosynostosis, the fusion occurs in one or both of the two sutures that run from the top of the ear to the top of the skull. These are known as the coronal sutures.
If only one coronal suture is fused, the infant will develop a flattened forehead on the affected side. They may also have a raised eye socket and a crooked nose. If both coronal sutures are fused, the infant will develop a flat and prominent forehead and brow.
Metopic synostosis is an uncommon type of craniosynostosis, occuring in 4-10% of cases. The fusion occurs in the metopic synostosis, which is the suture that runs from the nose to the top of the skull. Infants with metopic synostosis will develop a pointed scalp that looks triangular.
Lambdoid synostosis is the rarest type of craniosynostosis and occurs in about 2-4% of cases. Fusion occurs in the lambdoid suture, which runs along the back of the head. Infants with lambdoid synostosis will develop a flattened head at the back.
However, not all children with a flattened head at the back have lambdoid synostosis. It is common and normal for babies to have some flatness at the back of their head as a result of lying on their backs for prolonged periods of time. This is known as positional plagiocephaly.

Bedwetting
Bedwetting is common in young children, but gets less common as children get older.
Most children respond well to treatment, although they may still wet the bed from time to time.
It’s best to try a few measures yourself first, such as:
not giving your child anything to drink in the hour before bedtime
making sure they have a wee before going to sleep
See some more self-help tips for bedwetting.
You could also consider buying a bedwetting alarm.
Reassure your child. It’s important for them to know they haven’t done anything wrong, and it will get better.
Don’t tell them off or punish them for wetting the bed as this won’t help and could make the problem worse.
Bedwetting is only really a problem if it begins to bother you or your child. It’s not usually considered a problem in children under five.
It’s a good idea to speak to your GP if:
your child has any other symptoms along with bedwetting, such as pain when weeing, fever or constipation
your child has suddenly started wetting the bed after they’ve been dry at night for a while
Lots of families first get medical help when the bedwetting affects a child’s social life – for example, if they don’t want to do sleepovers in case they wet the bed.
Your doctor may recommend a bedwetting alarm. These are moisture-sensitive pads your child wears on their night clothes. An alarm sounds if they start to wee.
You may be able to borrow an alarm from your local incontinence or enuresis clinic.
If an alarm doesn’t work or isn’t suitable, medicines for bedwetting may help. Medical treatments aren’t usually recommended for children under five.
Read more about treating bedwetting.
There’s usually no obvious reason why children wet the bed, but it could be because your child:
produces more wee than their bladder can cope with
has an overactive bladder, meaning it can only hold a small amount of wee
is a very deep sleeper, so they don’t react to the signals telling their brain their bladder is full
Bedwetting often runs in families.
Constipation is often linked with bedwetting. Sometimes treating constipation is all that’s needed to treat bedwetting.
Occasionally, bedwetting is triggered by emotional distress, such as being bullied or moving to a new school.
In rare cases, bedwetting may be a symptom of an underlying health condition, such as type 1 diabetes.
Read more about the causes of bedwetting.

Multiple system atrophy
Multiple system atrophy is a rare nervous system disorder where nerve cells in several parts of the brain deteriorate over time.
This causes problems with balance, movement and the autonomic nervous system, which controls a number of the body’s automatic functions, such as breathing and bladder control.
Symptoms of multiple system atrophy usually start when someone is between 50 and 60 years of age, but they can come at any time after 30.
The symptoms are wide-ranging and include muscle control problems, similar to those of Parkinson’s disease.
Many different functions of the body can be affected, including the urinary system, blood pressure control and muscle movement.
Although there are many different possible symptoms of multiple system atrophy, not everyone who’s affected will have all of them.
Men and women with multiple system atrophy will usually have one or more of the following bladder symptoms:
constantly feeling the need to pee
peeing more frequently
being unable to empty the bladder properly
being unable to pee
Men with multiple system atrophy will usually experience erectile dysfunction (the inability to get and maintain an erection), although this is a common problem that many men without the condition develop.
Someone with multiple system atrophy will often feel lightheaded, dizzy and faint after standing up. This is known as postural hypotension and is caused by a drop in blood pressure when they stand upright.
When you stand up after lying down, your blood vessels usually narrow quickly and your heart rate increases slightly to prevent your blood pressure from dropping and decreasing blood flow to your brain.
This function is carried out automatically by the autonomic nervous system; however, this system doesn’t work properly in people with multiple system atrophy, so the control is lost.
In multiple system atrophy, a part of the brain called the cerebellum is damaged. This can make the person clumsy and unsteady when walking, and can also cause slurred speech.
These problems are collectively known as cerebellar ataxia.
A person with multiple system atrophy has much slower movements than normal (bradykinesia). This can make it difficult to carry out everyday tasks. Movement is hard to initiate, and the person will often have a distinctive slow, shuffling walk with very small steps.
Some people may also have stiff, tense muscles. This can make it even more difficult to move around and cause painful muscle cramps (dystonia).
The above symptoms are typical of Parkinson’s disease but, unfortunately, the medication used to relieve them in people with Parkinson’s disease (levodopa) isn’t very effective for people with multiple system atrophy.
People with multiple system atrophy may also have:
cold hands and feet
problems controlling sweating
muscle weakness in the body and limbs – it may be more pronounced in one arm or leg
uncontrollable laughing or crying
sleep problems – insomnia, snoring, restless legs or nightmares
noisy breathing and unintentional sighing
a weak, quiet voice
blurred vision
dementia (although this is uncommon)
The causes of multiple system atrophy aren’t well understood.
It doesn’t appear to be inherited – there’s no evidence that an affected person’s children will develop it.
However, it’s possible that both genetic and environmental factors may contribute, so research is currently looking at whether there’s a genetic tendency (predisposition) to develop it.
The brain cells of a person with multiple system atrophy contain a protein called alpha-synuclein. A build-up of abnormal alpha-synuclein is thought to be responsible for damaging areas of the brain that control balance, movement and the body’s autonomic functions.
There’s no specific test to diagnose multiple system atrophy.
A diagnosis can usually be made based on the symptoms, although it can potentially be confused with Parkinson’s disease.
A person is more likely to have multiple system atrophy rather than Parkinson’s disease if:
their symptoms have progressed rapidly – a person with Parkinson’s disease deteriorates more slowly
they’ve experienced falls in the early stages of the condition – this isn’t a typical symptom of Parkinson’s
they don’t respond well to levodopa therapy – levodopa can significantly improve symptoms of Parkinson’s disease
their speech is severely affected – this isn’t a typical symptom of Parkinson’s disease
they gasp and breathe noisily – this isn’t a typical symptom of Parkinson’s disease
If multiple system atrophy is suspected, a doctor (usually a neurologist) will test the person’s reflexes and “automatic” bodily functions, such as their bladder function.
A brain scan is often needed – usually an MRI scan or a SPECT scan – to detect any loss of brain cells. Read more about SPECT scans (PDF, 304kb).
More detailed assessments of autonomic function may also be carried out – for example, recording blood pressure changes when lying down and standing.
There’s currently no cure for multiple system atrophy and no way of slowing its progression.
People with the condition typically live for six to nine years after their symptoms start and may deteriorate quickly during this time. Some people may live for more than 10 years after being diagnosed.
Help and support is available, and the symptoms can be managed so that the person is as independent and comfortable as possible.
Read about the:
treatment of low blood pressure
treatment of urinary incontinence
treatment of swallowing problems
Physiotherapy and occupational therapy can help people with multiple system atrophy stay mobile and maintain fitness and muscle strength.
Practical and financial help is available if you care for someone with multiple system atrophy.
Your local authority can carry out a carers’ assessment to assess your needs and determine the help and support you’re entitled to.
Find out more about carers’ assessments.
If you have multiple system atrophy and are finding coping with day-to-day life difficult, your doctor or nurse can refer you to a social worker.
They can carry out an assessment and recommend the help you require. For example, you may need:
care attendants – who can help with everyday tasks such as housework, dressing and washing
meals on wheels – your local council may be able to offer financial help for this; check your eligibility for getting meals at home
benefits – you may be eligible for a number of benefits, such as Attendance Allowance and Personal Independence Payment (PIP)
home adaptations – to make moving around at home easier and ensure your home environment is as comfortable as possible
Find out more about care and support needs assessments.

What is Treacher Collins syndrome?
What is Treacher Collins syndrome?
This video introduces you to this rare genetic condition!