Klinefelter syndrome
Introduction
Klinefelter syndrome (sometimes called Klinefelter’s, KS or XXY) is where boys and men are born with an extra X chromosome.
Chromosomes are packages of genes found in every cell in the body. Two types of chromosome, called the sex chromosomes, determine the genetic sex of a baby. These are named either X or Y.
Usually, a female baby has two X chromosomes (XX) and a male has one X and one Y (XY). But in Klinefelter syndrome, a boy is born with an extra copy of the X chromosome (XXY).
The X chromosome is not a “female” chromosome and is present in everyone. The presence of a Y chromosome denotes male sex.
Boys and men with Klinefelter syndrome are still genetically male, and often will not realise they have this extra chromosome, but occasionally it can cause problems that may require treatment.
Klinefelter syndrome is quite common, affecting around 1 in every 660 males.
Symptoms of Klinefelter syndrome
Klinefelter syndrome doesn’t usually cause any obvious symptoms early in childhood, and even the later symptoms may be difficult to spot.
Many boys and men don’t realise they have it.
-
in babies and toddlers – learning to sit up, crawl, walk and talk later than usual, being weaker, quieter and more passive than usual
in childhood – shyness and low self-confidence, problems with reading, writing, spelling and paying attention, mild dyslexia and/or dyspraxia, low energy levels, difficulty socialising or expressing feelings
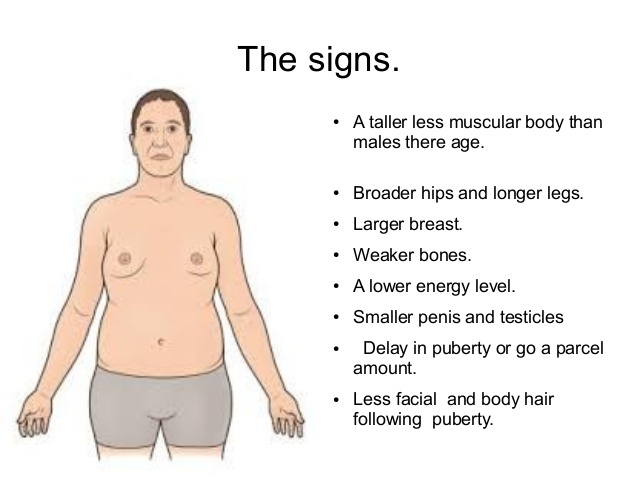
in teenagers – growing taller than expected for the family (with long arms and legs), broad hips, poor muscle tone and slower than usual muscle growth, reduced facial and body hair that starts growing later than usual, a small penis and testicles, enlarged breasts (gynaecomastia)
in adulthood – inability to have children naturally (infertility) and a low sex drive, in addition to the physical characteristics mentioned above
Health issues in Klinefelter syndrome
Most boys and men with Klinefelter syndrome will not be significantly affected and can live normal, healthy lives.
Infertility tends to be the main problem, although there are treatments that can help (see Treatments below).
However, men with Klinefelter syndrome are at a slightly increased risk of developing other health problems, including:
weak and fragile bones (osteoporosis)
cardiovascular disease and blood clots
autoimmune disorders (where the immune system mistakenly attacks the body), such as lupus
an underactive thyroid gland (hypothyroidism)
anxiety, learning difficulties and depression – although intelligence is usually unaffected
male breast cancer – although this is very rare
These problems can usually be treated if they do occur and testosterone replacement therapy may help reduce the risk of some of them.
Causes of Klinefelter syndrome
Klinefelter syndrome is caused by an additional X chromosome.
This chromosome carries extra copies of genes, which interfere with the development of the testicles and mean they produce less testosterone (male sex hormone) than usual.
The extra genetic information may either be carried in every cell in the body or it may only affect some cells (known as mosaic Klinefelter syndrome).
Klinefelter syndrome isn’t directly inherited – the additional X chromosome occurs as a result of either the mother’s egg or the father’s sperm having the extra X chromosome (an equal chance of this happening in either), so after conception the chromosome pattern is XXY rather than XY.
This change in the egg or sperm seems to happen randomly. If you have a son with the condition, the chances of this happening again are very small.
However, the risk of a woman having a son with Klinefelter syndrome may be slightly higher if the mother is over 35 years of age.
Testing for Klinefelter syndrome
See your GP if you have concerns about your son’s development or you notice any troubling symptoms of Klinefelter syndrome in yourself or your son.
Klinefelter syndrome isn’t necessarily anything serious, but treatment can help reduce some of the symptoms if necessary.
In many cases, it’s only detected if a man with the condition undergoes fertility tests.
Your GP may suspect Klinefelter syndrome after a physical examination and they may suggest sending off a sample of blood to check reproductive hormone levels.
The diagnosis can be confirmed by checking a sample of blood for the presence of the extra X chromosome.
Treatments for Klinefelter syndrome
There’s no cure for Klinefelter syndrome, but some of the problems associated with the condition can be treated if necessary.
Possible treatments include:
testosterone replacement therapy (see below)
speech and language therapy during childhood to help with speech development
educational and behavioural support at school to help with any learning difficulties or behaviour problems
occupational therapy to help with any co-ordination problems associated with dyspraxia
physiotherapy to help build muscle and increase strength
psychological support for any mental health issues
fertility treatment – options include artificial insemination using donor sperm or possibly intra-cytoplasmic sperm injection (ICSI), where sperm removed during a small operation are used to fertilise an egg in a laboratory
breast reduction surgery to remove excess breast tissue
Testosterone replacement therapy
TRT involves taking medication containing testosterone. It can be taken in the form of gels or tablets in teenagers, or given as gel or injections in adult men.
TRT may be considered once puberty begins and may help with the development of a deep voice, facial and body hair, an increase in muscle mass, reduction in body fat, and improvement in energy. You should see a specialist in children’s hormones (a paediatric endocrinologist) at this time.
Long-term treatment during adulthood may also help with several other problems associated with Klinefelter syndrome – including osteoporosis, low mood, reduced sex drive, low self-esteem and low energy levels – although it can’t reverse infertility.
More information and support
If you or your son has been diagnosed with Klinefelter syndrome, you might find it useful to find out more about it and get in touch with others affected by it.
The following websites may be able to help:


