An international team has shown that the injection of a type of stem cell into the brains of patients living with progressive multiple sclerosis (MS) is safe, well tolerated and has a long-lasting effect that appears to protect the brain from further damage.
The study, led by scientists at the University of Cambridge, University of Milan Bicocca and Hospital Casa Sollievo della Sofferenza (Italy), is a step towards developing an advanced cell therapy treatment for progressive MS.
Over 2 million people live with MS worldwide, and while treatments exist that can reduce the severity and frequency of relapses, two-thirds of MS patients still transition into a debilitating secondary progressive phase of disease within 25-30 years of diagnosis, where disability grows steadily worse.
In MS, the body’s own immune system attacks and damages myelin, the protective sheath around nerve fibres, causing disruption to messages sent around the brain and spinal cord.
Key immune cells involved in this process are macrophages (literally ‘big eaters’), which ordinarily attack and rid the body of unwanted intruders. A type of macrophage known as a microglial cell is found throughout the brain and spinal cord. In progressive forms of MS, they attack the central nervous system (CNS), causing chronic inflammation and damage to nerve cells.
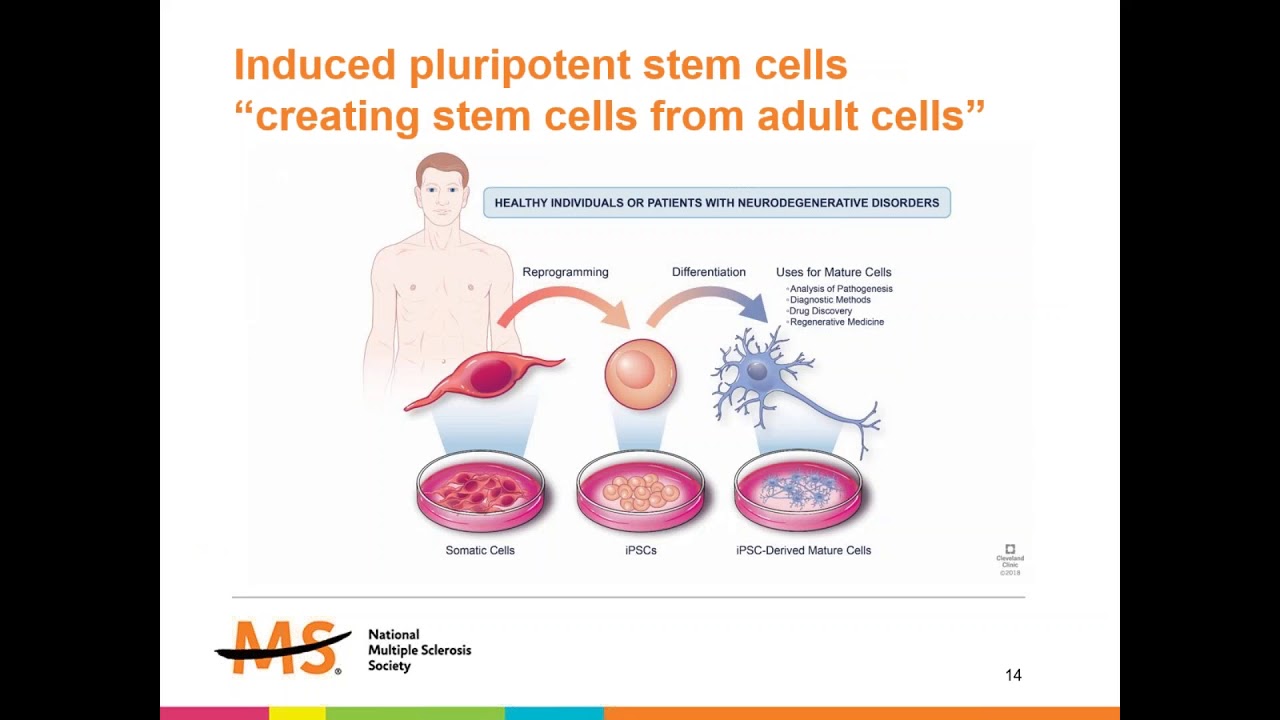
Recent advances have raised expectations that stem cell therapies might help ameliorate this damage. These involve the transplantation of stem cells, the body’s ‘master cells’, which can be programmed to develop into almost any cell type within the body.
Previous work from the Cambridge team has shown in mice that skin cells re-programmed into brain stem cells, and transplanted into the central nervous system, can help reduce inflammation and may be able to help repair damage caused by MS.
Now, in research published in the Cell Stem Cell, scientists have completed a first-in-man, early-stage clinical trial that involved injecting neural stem cells directly into the brains of 15 patients with secondary MS recruited from two hospitals in Italy. The trial was conducted by teams at the University of Cambridge, Milan Bicocca and the Hospitals Casa Sollievo della Sofferenza and S. Maria Terni (IT) and Ente Ospedaliero Cantonale (Lugano, Switzerland) and the University of Colorado (USA).
The stem cells were derived from cells taken from brain tissue from a single, miscarried foetal donor. The Italian team had previously shown that it would be possible to produce a virtually limitless supply of these stem cells from a single donor – and in future it may be possible to derive these cells directly from the patient – helping to overcome practical problems associated with the use of allogeneic foetal tissue.
The team followed the patients over 12 months, during which time they observed no treatment-related deaths or serious adverse events. While some side-effects were observed, all were either temporary or reversible.
All the patients showed high levels of disability at the start of the trial – most required a wheelchair, for example – but during the 12 month follow up period none showed any increase in disability or a worsening of symptoms. None of the patients reported symptoms that suggested a relapse and nor did their cognitive function worsen significantly during the study. Overall, say the researchers, this points to a substantial stability of the disease, without signs of progression, though the high levels of disability at the start of the trial make this difficult to confirm.
The researchers assessed a subgroup of patients for changes in the volume of brain tissue associated with disease progression. They found that the larger the dose of injected stem cells, the smaller the reduction in this brain volume over time. They speculate that this may be because the stem cell transplant dampened inflammation.
The team also looked for signs that the stem cells were having a neuroprotective effect – protecting nerve cells from further damage. Their previous work showed how tweaking metabolism – how the body produces energy – can reprogram microglia from ‘bad’ to ‘good’. This new study looked at how the brain’s metabolism changes after the treatment. They measured changes in the fluid around the brain and in the blood over time and found certain signs linked to how the brain processes fatty acids. These signs were connected to how well the treatment works and how the disease develops. The higher the dose of stem cells, the greater the levels of fatty acids, which also persisted over the 12-month period.
Professor Stefano Pluchino from the University of Cambridge, who co-led the study, said: “We desperately need to develop new treatments for secondary progressive MS, and I am cautiously very excited about our findings, which are a step towards developing a cell therapy for treating MS.
“We recognise that our study has limitations – it was only a small study and there may have been confounding effects from the immunosuppressant drugs, for example – but the fact that our treatment was safe and that its effects lasted over the 12 months of the trial means that we can proceed to the next stage of clinical trials.”
Co-leader Professor Angelo Vescovi from the University of Milano-Bicocca said: “It has taken nearly three decades to translate the discovery of brain stem cells into this experimental therapeutic treatment This study will add to the increasing excitement in this field and pave the way to broader efficacy studies, soon to come.”
Caitlin Astbury, Research Communications Manager at the MS Society, says: “This is a really exciting study which builds on previous research funded by us. These results show that special stem cells injected into the brain were safe and well-tolerated by people with secondary progressive MS. They also suggest this treatment approach might even stabilise disability progression. We’ve known for some time that this method has the potential to help protect the brain from progression in MS.
“This was a very small, early-stage study and we need further clinical trials to find out if this treatment has a beneficial effect on the condition. But this is an encouraging step towards a new way of treating some people with MS.”