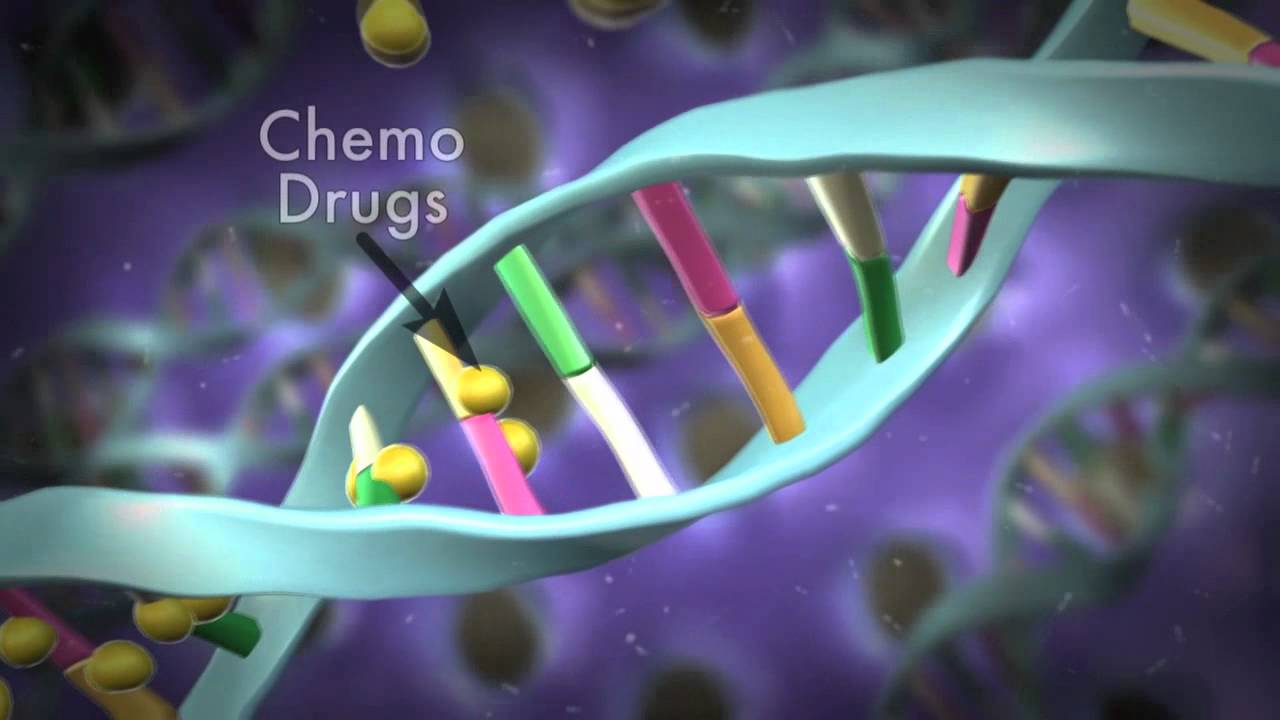
How Cells Divide and How Chemotherapy Works
How Cells Divide and How Chemotherapy Works. Learn more about this cancer treatment in this important video! For more on radiotherapy as a cancer treatment please go here.
How Cells Divide and How Chemotherapy Works
How Cells Divide and How Chemotherapy Works. Learn more about this cancer treatment in this important video! For more on radiotherapy as a cancer treatment please go here.

Radiotherapy
Radiotherapy is a treatment where radiation is used to kill cancer cells.
There are many different ways you can have radiotherapy, but they all work in a similar way.
They damage cancer cells and stop them from growing or spreading in the body.
Radiotherapy may be used in the early stages of cancer or after it has started to spread.
It can be used to:
try to cure the cancer completely (curative radiotherapy)
make other treatments more effective – for example, it can be combined with chemotherapy (chemoradiation) or used before surgery (neo-adjuvant radiotherapy)
reduce the risk of the cancer coming back after surgery (adjuvant radiotherapy)
relieve symptoms if a cure isn’t possible (palliative radiotherapy)
Radiotherapy is generally considered the most effective cancer treatment after surgery, but how well it works varies from person to person.
Ask your doctors about the chances of treatment being successful for you.
Radiotherapy can be given in several ways. Your doctors will recommend the best type for you.
The most common types are:
radiotherapy given by a machine (external radiotherapy) - where a machine is used to carefully aim beams of radiation at the cancer
radiotherapy implants (brachytherapy) - where small pieces of radioactive metal are (usually temporarily) placed inside your body near the cancer
radiotherapy injections, capsules or drinks (radioisotope therapy) - where radioactive liquid is swallowed or injected into your blood
Treatment is usually given in hospital. You can normally go home soon after external radiotherapy, but you may need to stay in hospital for a few days if you have implants or radioisotope therapy.
Most people have several treatment sessions, which are typically spread over the course of a few weeks.
Read more about what happens during radiotherapy.
As well as killing cancer cells, radiotherapy can damage some healthy cells in the area being treated.
This can cause some side effects, such as:
sore, red skin
feeling tired most of the time
hair loss in the area being treated
feeling sick
losing your appetite
a sore mouth
Many of these side effects can be treated or prevented and most will pass after treatment stops.
External radiotherapy doesn't make you radioactive, as the radiation passes through your body.
The radiation from implants or injections can stay in your body for a few days, so you may need to stay in hospital and avoid close contact with other people for a few days as a precaution.
Read more about the side effects of radiotherapy.
Growth hormone complications
Acromegaly is a condition in which the body produces too much growth hormone, leading to the excess growth of body tissues over time.
Typical features include:
Growth hormone is produced and released by the pituitary gland, a pea-sized gland just below the brain.
When growth hormone is released into the blood, it stimulates the liver to produce another hormone – insulin-like growth factor 1 (IGF-1) – which causes growth of muscle, bones and cartilage throughout the body.
This process is essential for growth and repair of body tissues.
Acromegaly is caused by excessive production of growth hormone.
This usually occurs as the result of a benign (non-cancerous) brain tumour in the pituitary gland called an adenoma, but rare cases have been linked to tumours elsewhere in the body, such as in the lungs and pancreas.
Although acromegaly does very occasionally run in families, most adenomas are not inherited – they usually develop spontaneously as a result of a genetic change within a cell of the pituitary gland. This genetic change switches on a signal that tells cells in the pituitary gland to divide and secrete growth hormone.
The tumour almost never spreads to other parts of the body, but it may grow to more than 1cm in size and compress the surrounding nerves and normal pituitary tissue, which can affect the production of other hormones, such as thyroid hormones released from the thyroid gland.
It’s not clear exactly how many people are affected by acromegaly, although it’s been estimated that around 4 to 13 in every 100,000 people may have the condition.
This means there is likely to be between 2,500 and 8,300 people in the UK with the condition.
Acromegaly can affect people of any age, but it is rare in children. The average age at which people are diagnosed is around 40-45.
Acromegaly can cause a wide range of symptoms that tend to develop slowly over time.
Typical symptoms include:
Some of the above symptoms are the result of the tumour compressing nearby tissues – for example, headaches and vision problems may occur if the tumour squashes nearby nerves.
If you think you have acromegaly, see your GP straight away. Acromegaly can usually be successfully treated with brain surgery and medication, but early diagnosis and treatment is important to prevent the symptoms getting worse and to reduce your chance of getting complications.
If acromegaly is left untreated, you may be at risk of the following health problems:
Left untreated, these complications can become serious and fatal.
If your doctor suspects acromegaly from your symptoms, they will order blood tests to measure your levels of human growth hormone.
Levels of growth hormone naturally vary from minute to minute as it is released from the pituitary gland in spurts. Therefore to accurately diagnose acromegaly, growth hormone needs to be measured under conditions that normally suppress growth hormone secretion.
To ensure an accurate result, you may be referred to a hospital doctor for a glucose tolerance test. This involves testing your blood after drinking a solution or drink containing the sugar glucose.
In most people, drinking the glucose solution will suppress the release of growth hormone, but in people with acromegaly, the level of growth hormone in the blood will remain elevated.
Your doctor will also measure your level of IGF-1, which should increase with the level of growth hormone. An elevated IGF-1 level almost always indicates acromegaly.
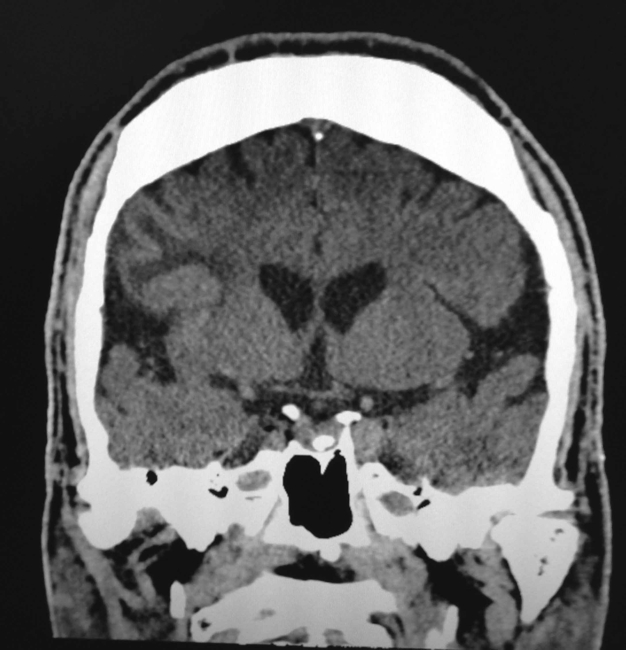
You may then have a magnetic resonance imaging (MRI) scan of your brain to locate and define the size of the pituitary gland tumour causing your acromegaly. A computerised tomography (CT) scan can be carried out if you are unable to have an MRI scan.
Treatment aims to:
This is usually achieved through surgical removal of the tumour and medication.
In most cases, surgery is recommended to remove the adenoma from your pituitary gland. This is effective in most people, although sometimes the tumour is too large to be removed completely.
Under a general anaesthetic, the surgeon will make an incision inside your nose or behind your upper lip to access the gland. An endoscope (a long, thin, flexible tube that has a light source and a video camera at one end) and surgical instruments are then passed through the incisions to remove the tumour.
Removing the tumour promptly relieves the pressure on the surrounding structures and leads to a rapid lowering of growth hormone levels. Facial appearance and swelling often improve within a few days.
Possible complications of surgery include damage to the healthy parts of the pituitary gland, leakage of cerebrospinal fluid (which surrounds and protects the brain), and meningitis, though this is rare. Your surgeon will discuss these risks with you and answer any questions you have.
Radiotherapy
If surgery is not possible, or surgery and medication do not cure the condition, radiotherapy aimed at the adenoma may be an option.
This can eventually lead to a reduction in growth hormone levels, although it may not have a noticeable effect for several years and you may need to take medication in the meantime.
There are two main types of radiotherapy for acromegaly:
Stereotactic radiosurgery is generally preferred to conventional radiotherapy because it minimises the risk of damage to nearby healthy tissue, although it is not always widely available.
Radiotherapy can have a number of side effects. For example, the treatment will often cause a gradual decline in the production of other hormones from your pituitary gland, so you’ll usually need to take hormone replacement therapy for the rest of your life. There’s also a risk it will impair fertility. Speak to your doctor about the risks involved.
There is some evidence acromegaly may increase your risk of bowel cancer, so guidelines recommend having a colonoscopy when you are diagnosed with the condition, and regular colonoscopy screening from the age of 40.
A colonoscopy is an examination of your entire large bowel using a type of endoscope called a colonoscope that is inserted into your bottom. See bowel cancer tests for more information about what a colonoscopy involves.
Treatment is often effective at stopping the excessive production of growth hormone and improving problems caused by the condition. Treatment can also increase life expectancy to around that of someone without acromegaly.
Some treatments can take a long time to have a noticeable effect and you may need to take medication for a long period of time.
After treatment, you’ll need regular follow-up appointments with your specialist for the rest of your life. These will be used to monitor your pituitary function, check you are on the correct hormone replacement treatment, and to ensure the condition does not return.
Without treatment, acromegaly can cause long-term problems and may reduce life expectancy by a number of years.
The purpose of this blog post is to provide a forum for people living with kidney cancer, also known
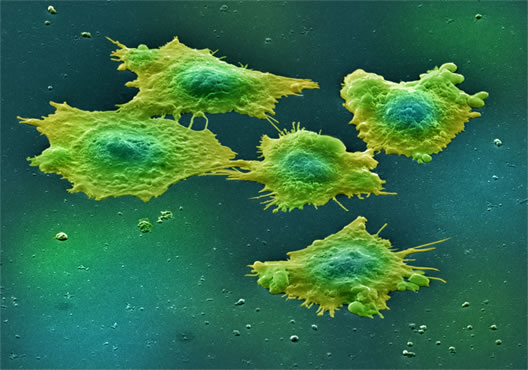
kidney cancer
Firstly what is kidney cancer? It is, in fact, the eighth most common cancer. Nearly 10,000 people are diagnosed with kidney cancer in the UK each year.
According to the UK’s NHS web site the signs and symptoms of kidney cancer can include:
However, they suggest that around 50% of people with kidney cancer do not present symptoms at an early stage and the disease is diagnosed via tests for other things. But during my career as a researcher I was told that, in fact, the figure is closer to 80% but I’ve not been able to get confirmation of this. If you have any information could you share it in the comments box please?
As always if you are in any way concerned about these symptoms it is vital that you see a healthcare professional as soon as possible.
Like many other cancers, kidney cancer is treated with chemotherapy, radiotherapy and surgery. Obviously various other medications can be used as well. MacMillan has a good overview which you can see here http://www.macmillan.org.uk/Cancerinformation/Cancertypes/Kidney/Treatingkidneycancer/Treatingkidneycancer.aspx
But, as we said, our main objective with this blog is to provide you with a forum to share your experience of kidney cancer. Either as a patient, a caregiver or family member.
Anything you have to say is of interest but you might wish to think about the following questions.
a) Can you tell us the story of your diagnosis. Who provided the diagnosis and when?
b) How did you and your family learn about the disease generally after the diagnosis?
c) What symptoms or events prompted your diagnosis of kidney cancer, if any?
d) What physicians/specialists have you seen in connection with your kidney cancer? Who do you see on an on-going basis?
e) How do you manage the disease on a daily basis?
Have you had to change your diet or lifestyle to cope with the disease?
f) What advice would you give to somebody who has just been diagnosed?
Please feel free to use the comments box below to share your kidney cancer journey.
Many thanks in advance.