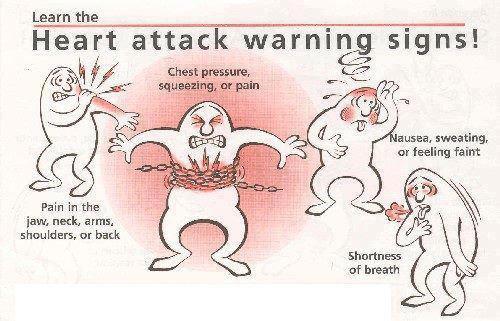
Heart Attack Warning Signs
The Cardiac Surgery Research team are conducting a series of trials into why almost half of patients having heart surgery develop failure of one or more other organs, such as the lungs or kidneys.
Organ failure after cardiac surgery is now causing higher rates of mortality nationally than breast cancer.
This vital new research relies on patients volunteering to take part in clinical trials, and members of the public, many of whom are heart attack survivors themselves, have volunteered their services to help cardiac surgery research by joining the ground-breaking Patient and Public Involvement (PPI) group.
The Cardiac Surgery Research PPI group is directly helping the research team’s work as it focuses on the possible side effects of blood transfusion and whether medicines used in other treatments might help prevent organ damage, as well as whether diseases like diabetes increase the likelihood of post-surgery complications occurring.
Silvia Marian told us : “Having members of the public cast an eye over the information we give to families whose children are about to undergo heart surgery, and whose help we are asking for in our research at such a difficult time for them, has been a huge help in getting the right messages across in the right way.”
A year ago the cardiac surgery team set up their PPI group to provide valuable feedback on what the studies’ priorities should be, to make sure that the research was relevant to patients themselves, to explain it clearly, and to raise awareness of this crucial work. They have also been active in organising events at which the researchers can talk about their work and its progress.
A central part of the PPI’s role is helping the research team by ensuring that the literature given to patients and their families is clear and easy to understand and that the volunteers themselves are fully supported throughout the trials.
The PPI team have arranged for Professor Gavin Murphy, BHF Professor of Cardiac Surgery at the University of Leicester and Consultant in Cardiac Surgery at Leicester’s Hospitals, to give a lecture entitled ‘How safe is blood transfusion?’ at Loughborough University on 16 June.
Commenting on the part played by his PPI group, Professor Murphy said: “By making public and patient participation part of our research strategy we will ensure that our research best reflects the needs and concerns of the community which it aims to help.
“We would be unable to deliver our current research strategy without the commitment and time kindly given by the previous patients and members of the public who make up our PPI, which is directly making a difference to both patient experience and research success to an unprecedented extent.”
Professor Murphy is celebrating the publication in the prestigious New England Journal of Medicine (NEJM) of his latest research paper on the effects of transfusion after cardiac surgery – details of which the PPI group will be helping to circulate at local events and through social media throughout the year.
