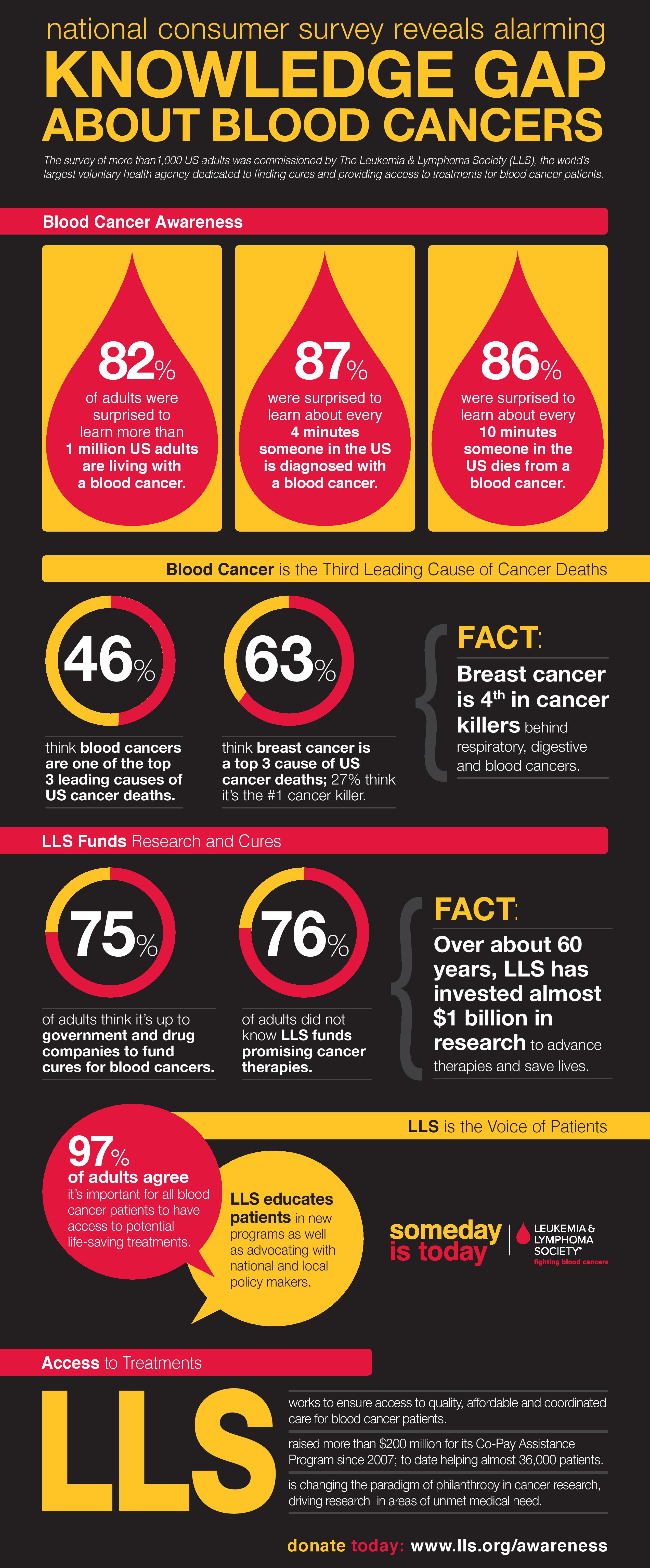
Blood Cancer Awareness
Doctors to be offered online training to improve UK’s poor diagnosis rates for blood cancers
• A new training course has been developed by blood cancer support charity Leukaemia CARE, in collaboration with the Royal College of General Practitioners (RCGP), and launched to mark the start of Blood Cancer Awareness Month
• The course set to radically improve GP knowledge of blood cancer symptoms, potentially saving around 1,000 lives a year
• Blood cancer survival from GP referral stands at 83.6% – but falls to 53.1% if diagnosis is delayed until the emergency admissions route.
• However, blood cancer symptoms can be easily confused with the symptoms of other less serious illnesses like the flu, leading to 33% of blood cancers – more than 10,000 patients – only diagnosed via emergency admissions
• Blood cancers such as leukaemia, lymphoma and myeloma are statistically the nation’s fifth largest cancer threat with 34,000 people diagnosed each year, and are the third biggest cancer killer
A new online training course designed to raise awareness of the symptoms of blood cancer among GPs is set to radically improve the rate of early diagnosis, bringing the UK up to EU standards and potentially saving around 1,000 lives a year.
Blood cancer support charity Leukaemia CARE, in collaboration with the Royal College of General Practitioners (RCGP), has developed the course in a bid to deliver better outcomes for the 34,000 people diagnosed with blood cancers in the UK each year.
When combined, blood cancers like leukaemia, lymphoma and myeloma are statistically the nation’s fifth largest cancer threat and third biggest cancer killer. And yet because many of the symptoms of blood cancer experienced by patients, such as persistent fatigue, night sweats, joint pain, bruising and recurrent infections, may also be linked with a wide range of other less serious diseases, 33% of blood cancers – more than 10,000 patients – are only diagnosed via the emergency admissions route, including accident and emergency.
Research shows that early diagnosis has a major impact on survival rates. For instance, the one year survival rate for myeloma patients diagnosed following a GP referral stands at 83.6% – but falls to 53.1% if diagnosis is delayed until the emergency admissions route3.
While online courses for GPs are available for other major cancers, this is the first of its kind for all blood cancers. Free of charge, it combines information on how to recognise the symptoms with case studies and, like all RCGP training courses, carries Continuous Professional Development (CPD) points – which GPs must complete to demonstrate that they are meeting the standards set by the General Medical Council.
The news comes as the UK marks its third Blood Cancer Awareness Month (1-30 September).
We interview Tony Gavin the Director of Campaigning and Advocacy at Leukaemia CARE and Dr Ishani Patel who is a GP and the Royal College of General Practitioners (RCGP) Clinical Lead for Early Diagnosis of Cancer and Quality Improvement
Question – What is blood cancer?

Dr Ishani Patel
Dr Ishani Patel – Blood cancer is an excessive growth of blood cells. For diseases such as lymphoma and leukaemia, this can be an excessive growth of white blood cells. The white blood cell is responsible for immunity and fighting off infection. However, when there is an overgrowth or an excessive amount of white cells, patients can often present with symptoms such as tiredness, excessive sweating, bone pains, bruising and bleeding. That’s a very brief overview of what a blood cancer is.
Question – How do leukaemia, lymphoma and myeloma differ from each other?
Tony Gavin – That is a huge question because within those disease areas there are also other disease types. There are 90 different leukaemias and 60 different lymphomas. There’s about 5 or 6 main types of myeloma, as well as other types, so we couldn’t really begin to describe the differences between them.
Collectively blood cancers are a huge problem in the UK and they are very poorly understood. At Leukaemia Care we think of them as a Cinderella disease, tucked away in the background with nobody fully aware of them, but blood cancers are the fourth largest notifiable cancer amongst men and women. Indeed if you look at the mortality rates and the people who die from blood cancer, more people die from blood cancer than die from breast cancer, more people die from blood cancer than die from prostate cancer. The sixth largest notifiable cancer in the UK is malignant melanoma (skin cancer). More people die from blood cancer than are actually diagnosed with skin cancer.
That’s how significant the problem is and that’s why we decided we needed to do something to help general practitioners recognise the signs and symptoms of the disease.
Question – What do the stages of different cancers mean?
Dr Ishani Patel – The different stages correspond with how much the disease has progressed.
For example in the context of blood cancers and the subset myeloma, if you present to the GP and are referred onto a specialist, your 1 year survival rate is 84% because you are diagnosed at an early stage, so stage 1.
However if you present as an emergency presentation, which is a third of all blood cancers, your 1 year survival rate drops to 55% so that’s a late stage diagnosis, which could be considered stage 3 or 4.
It’s difficult to drill into the detail of what each stage means because it’s obviously different depending on the type of blood cancer and as Tony’s just mentioned there are over 100 different types of blood cancers just within that terminology.
Question – What are the early signs and symptoms of blood cancers?
Dr Ishani Patel – Signs and symptoms to look out for include tiredness, excessive sweating, bone pain, bruising, bleeding, and recurrent infections. These can all present as individual signs or as a cluster of an early blood cancer. However if patients experience loss of appetite or weight loss, those are obviously signs of perhaps a cancer that has progressed.
Tony Gavin – With the lymphomas for instance you might have lumps in the neck or lumps in the armpit, or lumps in the groin. And the other thing to look out for is that quite a lot of the symptoms can be defined by something else. They could be just a common cold or flu or even menopause for the older patient. It’s when these signs and symptoms are persistent that you really need to take notice of them.
Question – Who treats these cancers and how?
Dr Ishani Patel – If we were to look at a classic patient journey, the GP who thinks there is a collection of symptoms that are causing concern would arrange for blood tests and perhaps a urine test or potentially even x-rays within primary care. They would arrange for what’s called a fast track cancer referral, which is a two-week-wait cancer referral where the patient can then be met by a haematologist. However, not all patients experience the same journey because of the varying ways that they present.
If a patient presents with, for example, a neck lump or a lump in their armpit or groin, they may go straight to a surgeon because they need to get a tissue sample or a biopsy to get a diagnosis.
However if a patient that presents with these symptoms then has a blood test and the blood test itself is abnormal, then they may be routed to a haematologist. Not everybody sees a haematologist straight away because it does very much depend on how they present in the first place.
Tony Gavin – The problem with bone pain is you would probably be referred to an orthopaedic surgeon before they realize it could be myeloma for instance. Within the blood cancer specialist community, within the haematology community, there are people that will specialise in leukaemias, lymphomas, and myelomas, and indeed within the leukaemias you may get people that specialise with chronic myeloid leukaemia, and those that specialize with acute myeloid leukaemia, so it varies. There are generalists and there are very, very specific specialists.
Question – How effective are the treatments?
Tony Gavin – That’s a really good question but a very difficult one to answer because you will find  different treatments for the whole range of different disease areas. I can quote one disease area where there is really, really good news. About 12 years ago survival rates for chronic myeloid leukaemia (CML) were poor. If you were diagnosed with CML in 2000 for instance then your survival prospects would be 3 – 5 years. In 2001 a new drug called Imatanib was developed – a tyrosine-kinase inhibitor. This class of drug has completely and utterly revolutionised the treatment of CML. Patients that respond to these drugs will not die from CML, they will not die from the leukaemia. This particular class of drugs is amazing, it’s one of the best good luck stories going around. It is a huge step change in the treatment of that particular disease.
different treatments for the whole range of different disease areas. I can quote one disease area where there is really, really good news. About 12 years ago survival rates for chronic myeloid leukaemia (CML) were poor. If you were diagnosed with CML in 2000 for instance then your survival prospects would be 3 – 5 years. In 2001 a new drug called Imatanib was developed – a tyrosine-kinase inhibitor. This class of drug has completely and utterly revolutionised the treatment of CML. Patients that respond to these drugs will not die from CML, they will not die from the leukaemia. This particular class of drugs is amazing, it’s one of the best good luck stories going around. It is a huge step change in the treatment of that particular disease.
Question – Please tell us about this new online tool, what it does and what its value will be.
Dr Ishani Patel – Leukaemia Care and the Royal College of General Practitioners have come together to develop a one hour learning course for not only GPs but all primary care health professionals. GPs are legally and professionally required to commit and evidence their own professional development i.e. the time they contribute to their own education. What Leukaemia Care has recognised is that the other cancers have a lot of attention both in the media and within GP education and we didn’t want blood cancers to be overlooked. So what this course does is provide case based scenarios almost like it is in real life. As a GP you’re sitting in your consultation room and a patient presents with a cluster of symptoms and it challenges the GP to think about what their next steps would be. For example if a patient presents with tiredness and with a lump in the neck what would they do next? And then once they have submitted their answers and evidenced their own reflection, it then takes them through to the gold standard and through the NICE guidelines on what they should do next, how to ensure rapid investigation and how to ensure that the patient’s route to diagnosis is as quick as possible.
Question – What one piece of advice would you give to someone who has just been diagnosed with a blood cancer?
Dr Ishani Patel – That’s a very tough question because there are different types of blood cancers. What I would say is that something that does get overlooked with all cancer treatments is nutrition. I would advise any patient going through or preparing to go through cancer treatments that could include steroids, chemotherapy, stem cell transplants and as Tony was saying tyrosine-kinase inhibitors that having a high protein diet and ensuring their nutrition is adequate will support them through their journey especially with managing the adverse effects of treatments. That would be my input from a GP perspective.
Tony Gavin – From my perspective, I would echo what Dr Patel has said but also say that they are not alone. They need to get in touch with a specialist organisation like Leukaemia Care, which can support them through their treatment. They can go online to leukaemiacare.org.uk and they can talk to our specialist nurse or talk to our care line experts. We have a care line that operates 24/7 so they can phone us at any time for help and advice and we can also put them in touch with patients who have been diagnosed with a similar disease so they can share their concerns and their worries. The other thing I have to say is there are breakthrough drugs coming through all the time in all the different disease areas and some of the new treatments coming through are superb. So first of all, don’t lose hope, get in touch with an organisation like Leukaemia Care and we’ll put you in touch with other groups too if you need to speak to somebody else.
We have a wealth of information online too and there’s lots that they can do to educate themselves on the disease.
Question – Where can people go for more information?
Dr Ishani Patel – Leukaemia Care provides robust information that is easy for patients to understand. From a GP perspective, I would encourage GPs to go to the Royal College of GPs website and do the online learning exercises to then be able to communicate that back to patients.
Tony Gavin – If patients do need more information once they have been in touch with Leukaemia Care, we can signpost them onto other areas.