
Time stamps:
0:29 What Causes Spasticity
1:32 Conservative Treatments
5:13 Drugs
7:20 Marijuana
8:43 Botox
10:49 Baclofen Pump
12:17 Other Treatments

Living near major roads or highways is linked to higher incidence of dementia, Parkinson’s disease, Alzheimer’s disease and multiple sclerosis (MS), suggests new research published this week in the journal Environmental Health.
Researchers from the University of British Columbia analyzed data for 678,000 adults in Metro Vancouver. They found that living less than 50 metres from a major road or less than 150 metres from a highway is associated with a higher risk of developing dementia, Parkinson’s, Alzheimer’s and MS–likely due to increased exposure to air pollution.
The researchers also found that living near green spaces, like parks, has protective effects against developing these neurological disorders.
“For the first time, we have confirmed a link between air pollution and traffic proximity with a higher risk of dementia, Parkinson’s, Alzheimer’s and MS at the population level,” says Weiran Yuchi, the study’s lead author and a PhD candidate in the UBC school of population and public health. “The good news is that green spaces appear to have some protective effects in reducing the risk of developing one or more of these disorders. More research is needed, but our findings do suggest that urban planning efforts to increase accessibility to green spaces and to reduce motor vehicle traffic would be beneficial for neurological health.”
Neurological disorders–a term that describes a range of disorders, including Alzheimer’s disease and other dementias, Parkinson’s disease, multiple sclerosis and motor neuron diseases–are increasingly recognized as one of the leading causes of death and disability worldwide. Little is known about the risk factors associated with neurological disorders, the majority of which are incurable and typically worsen over time.
For the study, researchers analyzed data for 678,000 adults between the ages of 45 and 84 who lived in Metro Vancouver from 1994 to 1998 and during a follow-up period from 1999 to 2003. They estimated individual exposures to road proximity, air pollution, noise and greenness at each person’s residence using postal code data. During the follow-up period, the researchers identified 13,170 cases of non-Alzheimer’s dementia, 4,201 cases of Parkinson’s disease, 1,277 cases of Alzheimer’s disease and 658 cases of MS.
For non-Alzheimer’s dementia and Parkinson’s disease specifically, living near major roads or a highway was associated with 14 per cent and seven per cent increased risk of both conditions, respectively. Due to relatively low numbers of Alzheimer’s and MS cases in Metro Vancouver compared to non-Alzheimer’s dementia and Parkinson’s disease, the researchers did not identify associations between air pollution and increased risk of these two disorders. However, they are now analyzing Canada-wide data and are hopeful the larger dataset will provide more information on the effects of air pollution on Alzheimer’s disease and MS.
When the researchers accounted for green space, they found the effect of air pollution on the neurological disorders was mitigated. The researchers suggest that this protective effect could be due to several factors.
“For people who are exposed to a higher level of green space, they are more likely to be physically active and may also have more social interactions,” said Michael Brauer, the study’s senior author and professor in the UBC school of population and public health. “There may even be benefits from just the visual aspects of vegetation.”
Brauer added that the findings underscore the importance for city planners to ensure they incorporate greenery and parks when planning and developing residential neighbourhoods.

Multiple system atrophy
Multiple system atrophy is a rare nervous system disorder where nerve cells in several parts of the brain deteriorate over time.
This causes problems with balance, movement and the autonomic nervous system, which controls a number of the body’s automatic functions, such as breathing and bladder control.
Symptoms of multiple system atrophy usually start when someone is between 50 and 60 years of age, but they can come at any time after 30.
The symptoms are wide-ranging and include muscle control problems, similar to those of Parkinson’s disease.
Many different functions of the body can be affected, including the urinary system, blood pressure control and muscle movement.
Although there are many different possible symptoms of multiple system atrophy, not everyone who’s affected will have all of them.
Men and women with multiple system atrophy will usually have one or more of the following bladder symptoms:
constantly feeling the need to pee
peeing more frequently
being unable to empty the bladder properly
being unable to pee
Men with multiple system atrophy will usually experience erectile dysfunction (the inability to get and maintain an erection), although this is a common problem that many men without the condition develop.
Someone with multiple system atrophy will often feel lightheaded, dizzy and faint after standing up. This is known as postural hypotension and is caused by a drop in blood pressure when they stand upright.
When you stand up after lying down, your blood vessels usually narrow quickly and your heart rate increases slightly to prevent your blood pressure from dropping and decreasing blood flow to your brain.
This function is carried out automatically by the autonomic nervous system; however, this system doesn’t work properly in people with multiple system atrophy, so the control is lost.
In multiple system atrophy, a part of the brain called the cerebellum is damaged. This can make the person clumsy and unsteady when walking, and can also cause slurred speech.
These problems are collectively known as cerebellar ataxia.
A person with multiple system atrophy has much slower movements than normal (bradykinesia). This can make it difficult to carry out everyday tasks. Movement is hard to initiate, and the person will often have a distinctive slow, shuffling walk with very small steps.
Some people may also have stiff, tense muscles. This can make it even more difficult to move around and cause painful muscle cramps (dystonia).
The above symptoms are typical of Parkinson’s disease but, unfortunately, the medication used to relieve them in people with Parkinson’s disease (levodopa) isn’t very effective for people with multiple system atrophy.
People with multiple system atrophy may also have:
cold hands and feet
problems controlling sweating
muscle weakness in the body and limbs – it may be more pronounced in one arm or leg
uncontrollable laughing or crying
sleep problems – insomnia, snoring, restless legs or nightmares
noisy breathing and unintentional sighing
a weak, quiet voice
blurred vision
dementia (although this is uncommon)
The causes of multiple system atrophy aren’t well understood.
It doesn’t appear to be inherited – there’s no evidence that an affected person’s children will develop it.
However, it’s possible that both genetic and environmental factors may contribute, so research is currently looking at whether there’s a genetic tendency (predisposition) to develop it.
The brain cells of a person with multiple system atrophy contain a protein called alpha-synuclein. A build-up of abnormal alpha-synuclein is thought to be responsible for damaging areas of the brain that control balance, movement and the body’s autonomic functions.
There’s no specific test to diagnose multiple system atrophy.
A diagnosis can usually be made based on the symptoms, although it can potentially be confused with Parkinson’s disease.
A person is more likely to have multiple system atrophy rather than Parkinson’s disease if:
their symptoms have progressed rapidly – a person with Parkinson’s disease deteriorates more slowly
they’ve experienced falls in the early stages of the condition – this isn’t a typical symptom of Parkinson’s
they don’t respond well to levodopa therapy – levodopa can significantly improve symptoms of Parkinson’s disease
their speech is severely affected – this isn’t a typical symptom of Parkinson’s disease
they gasp and breathe noisily – this isn’t a typical symptom of Parkinson’s disease
If multiple system atrophy is suspected, a doctor (usually a neurologist) will test the person’s reflexes and “automatic” bodily functions, such as their bladder function.
A brain scan is often needed – usually an MRI scan or a SPECT scan – to detect any loss of brain cells. Read more about SPECT scans (PDF, 304kb).
More detailed assessments of autonomic function may also be carried out – for example, recording blood pressure changes when lying down and standing.
There’s currently no cure for multiple system atrophy and no way of slowing its progression.
People with the condition typically live for six to nine years after their symptoms start and may deteriorate quickly during this time. Some people may live for more than 10 years after being diagnosed.
Help and support is available, and the symptoms can be managed so that the person is as independent and comfortable as possible.
Read about the:
treatment of low blood pressure
treatment of urinary incontinence
treatment of swallowing problems
Physiotherapy and occupational therapy can help people with multiple system atrophy stay mobile and maintain fitness and muscle strength.
Practical and financial help is available if you care for someone with multiple system atrophy.
Your local authority can carry out a carers’ assessment to assess your needs and determine the help and support you’re entitled to.
Find out more about carers’ assessments.
If you have multiple system atrophy and are finding coping with day-to-day life difficult, your doctor or nurse can refer you to a social worker.
They can carry out an assessment and recommend the help you require. For example, you may need:
care attendants – who can help with everyday tasks such as housework, dressing and washing
meals on wheels – your local council may be able to offer financial help for this; check your eligibility for getting meals at home
benefits – you may be eligible for a number of benefits, such as Attendance Allowance and Personal Independence Payment (PIP)
home adaptations – to make moving around at home easier and ensure your home environment is as comfortable as possible
Find out more about care and support needs assessments.

Lambert-Eaton myasthenic syndrome
Lambert-Eaton myasthenic syndrome (LEMS) is a very rare condition that affects the signals sent from the nerves to the muscles.
It means the muscles are unable to tighten (contract) properly, resulting in muscle weakness and a range of other symptoms.
About half of LEMS cases occur in middle-aged or older people with lung cancer. The remaining cases aren’t associated with cancer and can start at any age.
LEMS is also known as myasthenic syndrome or Eaton-Lambert syndrome.
The symptoms of LEMS develop gradually over weeks or months.
The main symptoms are weakness in the legs, arms, neck and face, as well as problems with automatic body functions, such as controlling blood pressure.
Common symptoms include:
aching muscles
difficulty walking and climbing stairs
difficulty lifting objects or raising the arms
drooping eyelids, dry eyes and blurred vision
dizziness upon standing
erectile dysfunction in men
strength that temporarily improves when exercising, only to reduce as exercise continues
See your GP if you have a combination of these symptoms.
LEMS is caused by the body’s natural defences (the immune system) mistakenly attacking and damaging the nerves.
Normally, nerve signals travel down the nerves and stimulate the nerve endings to release a chemical called acetylcholine. This chemical then helps activate the muscles.
If the nerve endings are damaged, the amount of acetylcholine they produce decreases, which means nerve signals don’t reach the muscles properly.
It’s not known what triggers the immune system to attack the nerves. It’s often associated with lung cancer, but can occur in people without cancer.
LEMS is not inherited.
Your GP will first check your medical history, ask about your symptoms, carry out a physical examination, and test your reflexes.
If they think you have a problem with your nerves, they may refer you to a specialist called a neurologist for further tests to determine the cause.
Tests you may have include:
blood tests – a blood test can detect substances in the blood (antibodies) resulting from the immune system attacking the nerves
nerve studies – a needle may be inserted into your skin to check how well signals are reaching the muscles from the nerves
scans – you may have a computerised tomography (CT) scan or positron emission tomography (PET) scan to check for lung cancer
If initial scans don’t find cancer, you may be advised to have regular scans every few months for a few years to check that it doesn’t develop later on.
There’s currently no cure for LEMS, but a number of treatments can help reduce the symptoms.
These include:
treatment for lung cancer – if you have lung cancer, treating it can significantly improve the symptoms of LEMS
medication to help nerve signals reach the muscles – commonly used medicines include 3,4-diaminopyridine and pyridostigmine
to reduce the activity of the immune system (immunosuppressants) – commonly used medicines include steroid tablets (prednisolone), azathioprine and methotrexate
immunoglobulin therapy – injections of antibodies from donated blood that temporarily stop your immune system attacking your nerves
plasmapheresis – a procedure to redirect your blood through a machine that filters out the antibodies attacking your nerves
Medication is the main treatment, although immunoglobulin therapy and plasmapheresis may be recommended in the short term, or if muscle weakness is severe and other treatments haven’t helped.
Some people respond well to treatment and are eventually able to stop taking medication, although this may not be for several years.
Others respond less well and find the condition affects their everyday activities and quality of life.
LEMS doesn’t affect life expectancy if it’s not associated with cancer. But people with lung cancer and LEMS tend to have a shorter life expectancy because it’s often not diagnosed until the cancer has spread, and by this point it’s very difficult to treat.
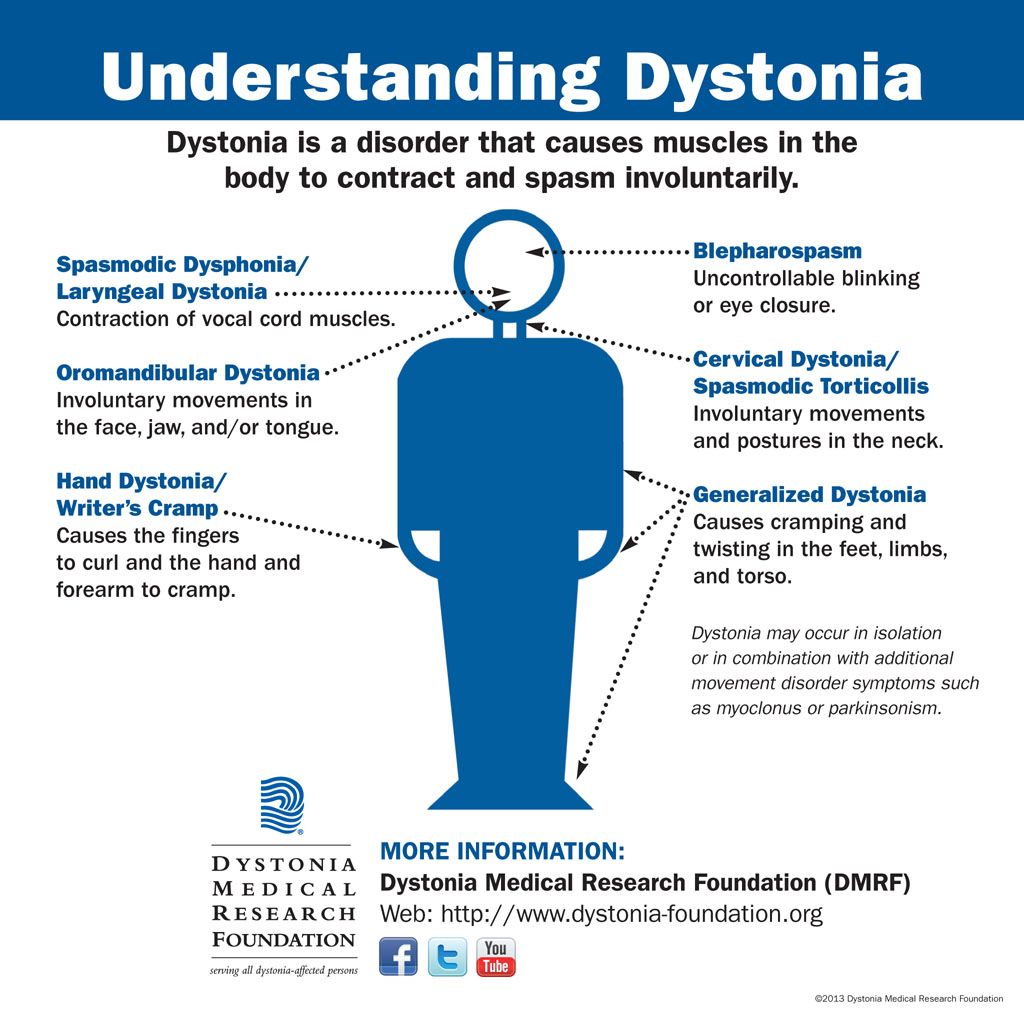
Dystonia
Dystonia is a medical term for a range of movement disorders that cause muscle spasms and contractions.
The spasms and contractions may either be sustained or may come and go.
Movements are often repetitive and cause unusual, awkward and sometimes painful postures. Tremor (shaking) can also be a characteristic of some types of dystonia.
Dystonia is thought to be a neurological condition (caused by underlying problems with the brain and nervous system). However, in most cases, brain functions such as intelligence, memory and language remain unaffected.
Dystonia can affect only one muscle or a group of muscles. There are five main types of dystonia:
Focal dystonia – where a single region, such as the hand or eyes, is affected. Cervical dystonia, blepharospasm (abnormal twitch of the eyelid), laryngeal dystonia and writer’s cramp are all examples of focal dystonia. If it only affects someone during specific activities, such as writing, it’s described as task-specific dystonia.
Segmental dystonia – where two or more connected regions of the body are affected. Cranial dystonia (blepharospasm affecting the lower face and jaw or tongue) is an example.
Multifocal dystonia – where two or more regions of the body that aren’t connected to each other, such as the left arm and left leg, are affected.
Generalised dystonia – where the trunk and at least two other parts of the body are affected. The legs may or may not be affected.
Hemidystonia – where one entire side of the body is affected.
About 90% of all cases are either cervical dystonia (which affects the neck muscles) or blepharospasm (which affects the eyelids). These are both focal dystonias that tend to develop later in life. They don’t usually get any worse and no other muscles are affected.
Read more about the symptoms of dystonia.
Exactly how dystonia develops remains uncertain, but it’s thought to be caused by a problem with the part of the brain that controls muscle movement (the basal ganglia).
If there’s no identifiable cause of dystonia, or if the cause is genetic, it’s described as primary dystonia.
Secondary dystonia is where dystonia occurs as a symptom of an underlying condition or injury. Common causes include stroke, brain injury, encephalitis and Parkinson’s disease.
Read more about the causes of dystonia.
Dystonia is diagnosed by a specialist examining and recognising the typical symptoms. The type of dystonia is then classified by which area of the body is affected.
When diagnosing dystonia, it’s important to confirm whether you have primary or secondary dystonia, because this may determine the type of treatment you need.
If you have typical signs of late-onset focal dystonia, specific investigations may not be required. However, tests may be needed to confirm whether you have primary or secondary dystonia. These may include brain scans, urine or blood tests, and genetic testing.
Read more about how dystonia is diagnosed.
There’s no cure for dystonia, but the condition can usually be effectively managed.
Treatment will vary, depending on the type of dystonia you have and the precise nature of your symptoms. However, the four main types of treatment are:
botulinum toxin – widely used to treat neurological conditions that involve abnormal muscle contractions, such as dystonia; it’s injected into the affected muscles to temporarily weaken them and reduce spasms
medication – such as anticholinergics, Baclofen and muscle relaxants
physiotherapy – where exercises are used to improve range of motion and posture, and prevent muscle weakness
surgery – if other treatments are unsuccessful, the nerves controlling the muscles causing spasms can be cut (selective peripheral denervation), or electrodes can be implanted within the brain, which are connected to a small device that’s similar to a pacemaker (deep brain stimulation)
Read more about how dystonia is treated.
Dystonia is an unpredictable condition. It tends to progress slowly and the severity of a person’s symptoms can vary from one day to another.
Focal dystonia usually progresses gradually over a period of about five years and then doesn’t get any worse.
Sometimes, a person’s symptoms improve or disappear completely. This is known as total remission and it’s thought to occur in around 5-10% of people.